Download
1 / 75
780 likes | 1.56k Views
Chapter Three. Teaching NANDA-I NIC and NOC: Novice to Exper t. Teaching NANDA-I NIC and NOC: Novice to Expert. Contributor Margaret Lunney. Explain Three Propositions Related to Teaching NNN Set Expectations for Students at Novice to Expert Stages of Development

E N D
Chapter Three Teaching NANDA-I NIC and NOC: Novice to Expert
Teaching NANDA-I NIC and NOC: Novice to Expert ContributorMargaret Lunney
Explain Three Propositions Related to Teaching NNN Set Expectations for Students at Novice to Expert Stages of Development Implement Teaching Strategies Integrate NNN With Nursing Curricula (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008) Learning Objectives
Objective 1: Explain Propositions • Use of NNN Requires Intellectual, Interpersonal, and Technical Competencies, Tolerance of Ambiguity and Reflection • Accurate Diagnoses are the Basis for Use of NIC and NOC • Use of NNN Differs from the Traditional Nursing Process (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Intellectual Knowledge Related to: Diagnoses Interventions Outcomes Thinking Processes Research Findings: Human Beings Vary in Thinking Process Abilities Thinking Process Abilities can be Improved Proposition #1: Skills/Competencies
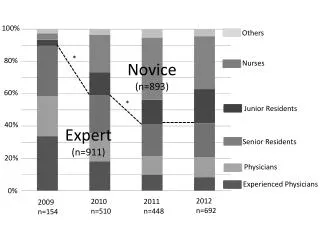
N = 86 (Lunney 1992) Variation in Nurses’ Thinking Abilities
Thinking Processes of Women Develop Through Relationships Women’s Perspectives on Thinking (Belenkey et al. 1986) Silence Received Knowledge Subjective Knowledge Procedural Knowledge Constructed Knowledge Nursing Students and Nurses may have Lower Level Perspectives Intellectual Skills Research Findings related to Women
Critical Thinking (CT) Processes can be Improved Stimulate to Use Expect Use Validate Appropriate Use Demonstrate Support and Confidence in Abilities CT Abilities - Essential for Accuracy of Diagnoses and Use of NOC and NIC (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008) Intellectual Skills: Critical Thinking
Delphi Study of 55 Nurse Experts (Scheffer and Rubenfeld 2000) Purpose: Identify the Components of CT that Relate to Nursing Results - Definition for Nursing: 7 Cognitive Skills 10 Habits of Mind Intellectual Skills: What is CT in Nursing?
Analyzing Applying Standards Discriminating Information Seeking Logical Reasoning Predicting Transforming Knowledge Cognitive Skills
Confidence Contextual Perspective Creativity Flexibility Inquisitiveness Intellectual Integrity Intuition Open-Mindedness Perseverance Reflection Habits of Mind
CT Involves Continuous Processing of Data and Inferences In Any Situation, Two or More Cognitive Skills are Probably Being Used Habits of Mind Support Cognitive Skills The Combination of CT Abilities Needed is Unique to the Situation Intellectual Skills: CT Process
Exquisite Communication Promote Trust Work n Partnership, Share Power Validate Perceptions Accept That We Do Not “Know” Others Proposition #1: Interpersonal Skills
Obtain Valid and Reliable Data Health Histories: Comprehensive Physical Exams: Focused Perform Nursing Interventions Technical Aspects of Using NNN Proposition #1: Technical Skills
Tolerate Ambiguity Decisions are Relative to Context and Specific Nature of Individuals Multiple Factors Influence Clinical Situations Human Beings are Complex and Diverse Ambiguity is the Norm Proposition #1: Personal Strengths
Reflect on Practice Experiences Accept Possible Flaws Thinking Interpersonal Technical Aim - Develop and Grow Proposition #1: Personal Strengths
Cues/Data may be Incorrect Examples Objective Data: Diagnostic Tests Subjective Data: Patients Families Proposition #2: Accurate Interpretations Foundational
Use of NNN Requires Many Decisions All Decisions are Based on Patient Data Data Amounts are Overwhelming Short-Term Memory = 7 ± 2 Bits of Data Data are Converted to Interpretations (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008) Proposition #2: Accurate Interpretations Foundational
Interpretations Determine Actions Additional Data Collection Subsequent Decisions Possible Outcomes to Consider Choices of Interventions High Potential for Inaccuracy Diagnosis and Etiology Proposition #2: Accurate Interpretations Foundational
(1) Marian Hughes is a 16-year-old girl with a medical diagnosis of diabetes mellitus. (2) She was admitted 3days ago for treatment of an acute episode of diabetic ketoacidosis. (3) When Marian discussed with you how she managed the therapeutic regimen before hospitalization, she states that she was not adhering to her prescribed diet. (4) You decide that Marian needs assistance to improve her management of the therapeutic regimen, especially the types of foods she eats. (5) Marian's stay in the hospital unit is uneventful in that medical treatments are successfully resolving the crisis. (6) Marian's daily habits include getting up for school about 7.00 a.m. and rushing to get the bus by 7.30. (7) She says that she should get up about 6.30 but she likes to sleep. (8) She states that she does not want her mother to help her get up earlier. (9) The meal that she eats at school is consistent with her prescribed diet while the two meals at home are not. (10) In the morning she grabs whatever is quick and easy, usually toast and butter. (11) In the evening, her mother makes meals that comply with the diabetic diet but Marian states that she does not like them so she only eats part of her supper and then snacks on other foods later. (12) Marian is able to explain to you what she should be eating and she can adjust her diet to her lifestyle. (13) The knowledge of what foods are on her diet that she likes was not discussed with her mother because she doesn't want to sit down and talk with her. (14) In general, Marian and her mother argue over many of Marian's behaviors, such as school grades, smoking, and coming in late at night. High Potential for Inaccuracy Case Study: Marian Hughes
16-Year-Old Diabetic (#1) Hospitalized, DKA (#2) “Did Not Follow Prescribed Diet” (#3) NDx: Ineffective Management of Therapeutic Regimen, Related to _______ (Fill in the Blank) High Potential for Inaccuracy Case Study: Marian Hughes
Knowledge Deficit Disconfirming Cues: Meals Eaten at School are Consistent with Diet (#9) Able to Explain What She Should be Eating (#12) She can Adjust Her Diet to Her Lifestyle (#13) Conclusion: Low Accuracy Diagnosis Teaching is Waste of Time, Effort, and Money High Potential for Inaccuracy Case Study: Marian HughesPossible Interpretation/Diagnosis (Herdman 2012)
Ineffective Self-Health Management, Related to Communication Difficulties Between Marian and Her Mother Patient Outcome (NOC): Communication = 3 (Moderately Compromised), Increase to 5 (Not Compromised) Nursing Intervention Communication Enhancement (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008) High Potential for Inaccuracy Case Study: Marian Hughes Highest Accuracy Diagnosis
Examples Communication Difficulties Mother/Daughter Stressful Mother/Child Relationship Altered Family Dynamics Ineffective Coping Ineffective Time Management Adolescent Image Low Self-Esteem Denial Deficient Knowledge 44 Diagnoses by 80 Nurses
+5 Highest Level of Accuracy +4 Close to the Highest Level But Not Quite +3 General Idea But Not Specific Enough +2 Not Enough Highly Relevant Cues or Not the Highest Priority +1 Suggested by Only One or a Few Cues 0 Not Indicated by Data -1 Should be Rejected, Disconfirming Cues Seven Levels of Accuracy
Communication Difficulties Between Mother and Daughter +5 Stressful Mother/Child Relationship +4 Altered Family Dynamics +3 Ineffective Coping +2 Ineffective Time Management +2 Adolescent Image +1 Low Self-Esteem +1 Denial 0 Deficient Knowledge -1 Diagnostic Accuracy Scores
Studies: 1966 to Present Conclusions: Interpretations Vary Widely All Interpretations are Not High Accuracy Influencing Factors (Carnevali 1983; Gordon 1982) Nurse Diagnostician Diagnostic Task Situational Context Research Findings
Diagnostic Task Lesser Amounts and Complexity of Data Nurse Diagnostician Education Related to Nursing Diagnoses Knowledge of Diagnostic Process and Concepts Teaching Aids for Diagnostic Reasoning Variety of Thinking Processes Experience Specific to Diagnostic Task Research: Positive Influences
Challenge: Achieving Accuracy Puzzle: What is the Diagnosis?
Supporting Factors: Acknowledge that Data Interpretations areProbabilistic; Question Accuracy Use CT, Interpersonal and Technical Skills Develop Tolerance ofAmbiguity It’s OK Not to Have an Answer Accept that We Might Make Mistakes Develop Reflective Practice Proposition #2: Accurate Interpretations Foundational
Traditional Limited # of Concepts Collect Comprehensive Data No Accountability for Diagnoses Intervene Based on Data Behavioral Outcomes Disorganized Follow-Up Use of NNN Currently 1147 Concepts Cue-Based and Hypothesis-Driven Data Collection Fully Accountable for Diagnoses Intervene Based on Data Interpretations Neutral Terms with Scale Systematic Follow-Up Proposition #2: New Perspectives on Nursing Process (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Acknowledge Difficulty Level: Simple to Complex Influencing Factors: Similarity of Terms in Three Systems Structure of Classifications Resources (Books, Pamphlets, Other) Complexity of Clinical Situations Nurses Perspective/Model for Practice Experience With NNN Changing from Traditional to Use of NNN (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Examples: User-Friendly Simplicity (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Use Theoretical Perspective Change Theory Diffusion of Innovations(Rogers 2003) S-Shaped Diffusion Curve Perceived Characteristics: Relative Advantage (+) Compatibility (+) Complexity (-) Trial Ability (+) Observability (+) Changing from Traditional to Use of NNN (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Be a Champion Sell First to Opinion Leaders Goal: Create a Critical Mass Share Demonstration Projects (For Example, Protocols and Journals) Faculty Development Program Adoption by System Adoption by Individuals Changing from Traditional to Use of NNN (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Novices and Advanced Beginners (ABS) Learn to Use NNN as Well as Experienced Nurses Novices and ABS may be Easier to Teach than Nurses at Competent, Proficient and Expert (Expert) Stages Expert Nurses must be “Sold” on New Way to Think and Document Objective 2: Set Expectations Novice to Expert (Benner 1984; Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
EHR is Imminent NNN = File Names for EHR NNN Describes What Nurses Bring to the Table NNN Makes Knowledge Available at Bedside Aggregated Data = Knowledge Measurement of Care = Improved Quality Linguistics Theory Supports SNLS Fits with Nursing Theories Selling NNN to Experts
Expect (At All Levels of Expertise): Correct Use of the Three Systems: Nursing Diagnoses are used to Guide Interventions, Not for Labeling per se Intervention Label is the Intervention, Not the Activities Outcome Label is the Outcome, Not the Indicators Correct Use of Concepts: NANDA-I: Social Isolation NIC: Coping Enhancement NOC: Knowledge (Specify) Set Expectations (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Do Not Underestimate Nursing Students or Nurses: “…Nursing and Nursing Knowledge must be Presented in All Its Complexity … Help Students and Nurses to “… Experience the Complex and Messy World of Nursing … and Learn How to Navigate Through It …” (Doane and Varcoe 2005, p.xi) Set Expectations
All Levels: Self-Evaluation Integrate with New Theories, for Example: Pender’s Health Promotion Model Integrate with Strategies for Evidence-Based Nursing Set Expectations (Pender et al. 2010)
Encourage Experts to: Integrate with Previous Knowledge Use NNN in: Communicating Scope of Practice Developing Standards of Care Evidence-Based Nursing Projects Research Projects Evaluate Clinical Applications of NNN Teach CE Programs to Nursing Personnel Set Expectations (Bulecheck et al. 2008; Herdman 2012; Moorhead et al. 2008)
Assume that Thinking Is Human, Imperfect, Attainable Encourage Thinking in Class and Clinical: Ask Questions Instead of Giving Answers Provide Opportunities for Problem Solving Objective 3: Teaching Strategies Intellectual
Objective 3: Teaching Strategies Intellectual: Deflate Authority
Think Out Loud with Students Act as Midwife or Coach Help them Think About Thinking: Ask: What Kind of Thinking is Needed? Use the 17 CT Terms and Definitions Evaluate Thinking Processes Expect Self-Evaluation of Thinking Objective 3: Teaching Strategies Intellectual
Share Paradigm Cases (e.g. Marian Hughes) Simplify Representations, Identify High Relevance Cues Conduct Iterative Hypothesis Testing Objective 3: Teaching Strategies
Seminars Instead of Lectures: Why? Groups Represent Wide Variations in Thinking Abilities Promotes “In-Class” Thinking Recognizes Students’ Abilities to Think and Learn without Authority/Experts Supports Future Work in Groups to Describe, Analyze and Synthesize Information, Solve Problems (e.g. What is the diagnosis?) Objective 3: Teaching Strategies Intellectual
Seminars: How? Assign Readings, Provide Discussion Questions Lead the Group, Ask the Discussion Questions Be Respectful; Protect Students’ Self-Esteem Address: What is the Author Saying? What is the Fit with Previous Knowledge? How Does This Information Apply to Practice? 25-30% of Grade for Discussion of Readings Objective 3: Teaching Strategies Intellectual
Expect Self Evaluation Ask Questions, Instead of Giving Answers Discussion in Class Discussion Online Journal Writing (Degazon and Lunney 1996) Objective 3: Teaching Strategies Intellectual
Expect Accountability For Patient Relationships Demonstrate: Good Interviewing Validation of Diagnoses Partnership Processes to Select Outcomes and Interventions Reward Power Sharing Teach and Support Assertiveness Objective 3: Teaching Strategies Interpersonal