Download
1 / 1
10 likes | 126 Views
V. C. U. Identifying Palliative Care Needs in the Emergency Department: Better Care, Lower Cost J Brian Cassel, PhD Laurie J Lyckholm, MD PO Box 980037 Richmond, VA 23298-0037. Background. Study 1. Study 2. Case Examples.

E N D
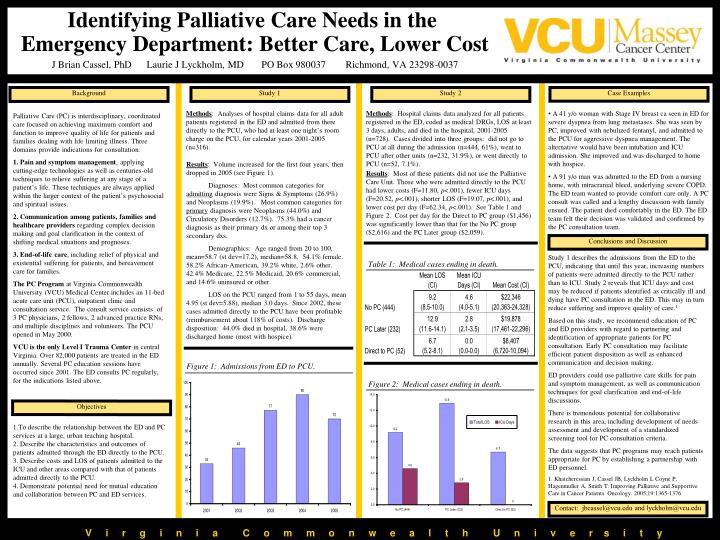
V C U Identifying Palliative Care Needs in the Emergency Department: Better Care, Lower Cost J Brian Cassel, PhD Laurie J Lyckholm, MD PO Box 980037 Richmond, VA 23298-0037 Background Study 1 Study 2 Case Examples Palliative Care (PC) is interdisciplinary, coordinated care focused on achieving maximum comfort and function to improve quality of life for patients and families dealing with life limiting illness. Three domains provide indications for consultation: 1.Pain and symptom management, applying cutting-edge technologies as well as centuries-old techniques to relieve suffering at any stage of a patient’s life. These techniques are always applied within the larger context of the patient’s psychosocial and spiritual issues. 2. Communication among patients, families and healthcare providers regarding complex decision making and goal clarification in the context of shifting medical situations and prognoses. 3.End-of-life care, including relief of physical and existential suffering for patients, and bereavement care for families. The PC Program at Virginia Commonwealth University (VCU) Medical Center includes an 11-bed acute care unit (PCU), outpatient clinic and consultation service. The consult service consists of 3 PC physicians, 2 fellows, 2 advanced practice RNs, and multiple disciplines and volunteers. The PCU opened in May 2000. VCU is the only Level I Trauma Center in central Virginia. Over 82,000 patients are treated in the ED annually. Several PC education sessions have occurred since 2001. The ED consults PC regularly, for the indications listed above. Methods: Analyses of hospital claims data for all adult patients registered in the ED and admitted from there directly to the PCU, who had at least one night’s room charge on the PCU, for calendar years 2001-2005 (n=316). Methods: Hospital claims data analyzed for all patients registered in the ED, coded as medical DRGs, LOS at least 3 days, adults, and died in the hospital, 2001-2005 (n=728). Cases divided into three groups: did not go to PCU at all during the admission (n=444, 61%), went to PCU after other units (n=232, 31.9%), or went directly to PCU (n=52, 7.1%). • A 41 y/o woman with Stage IV breast ca seen in ED for severe dyspnea from lung metastases. She was seen by PC, improved with nebulized fentanyl, and admitted to the PCU for aggressive dyspnea management. The alternative would have been intubation and ICU admission. She improved and was discharged to home with hospice. • A 91 y/o man was admitted to the ED from a nursing home, with intracranial bleed, underlying severe COPD. The ED team wanted to provide comfort care only. A PC consult was called and a lengthy discussion with family ensued. The patient died comfortably in the ED. The ED team felt their decision was validated and confirmed by the PC consultation team. Results: Volume increased for the first four years, then dropped in 2005 (see Figure 1). Diagnoses: Most common categories for admitting diagnosis were Signs & Symptoms (26.9%) and Neoplasms (19.9%). Most common categories for primary diagnosis were Neoplasms (44.0%) and Circulatory Disorders (12.7%). 75.3% had a cancer diagnosis as their primary dx or among their top 3 secondary dxs. Demographics: Age ranged from 20 to 100, mean=58.7 (st dev=17.2), median=58.8. 54.1% female. 58.2% African-American, 39.2% white, 2.6% other. 42.4% Medicare, 22.5% Medicaid, 20.6% commercial, and 14.6% uninsured or other. LOS on the PCU ranged from 1 to 55 days, mean 4.95 (st dev=5.88), median 3.0 days. Since 2002, these cases admitted directly to the PCU have been profitable (reimbursement about 118% of costs). Discharge disposition: 44.0% died in hospital, 38.6% were discharged home (most with hospice). Results: Most of these patients did not use the Palliative Care Unit. Those who were admitted directly to the PCU had lower costs (F=11.80, p<.001), fewer ICU days (F=20.52, p<.001), shorter LOS (F=19.07, p<.001), and lower cost per day (F=62.34, p<.001). See Table 1 and Figure 2. Cost per day for the Direct to PC group ($1,456) was significantly lower than that for the No PC group ($2,616) and the PC Later group ($2,059). Conclusions and Discussion Study 1 describes the admissions from the ED to the PCU, indicating that until this year, increasing numbers of patients were admitted directly to the PCU rather than to ICU. Study 2 reveals that ICU days and cost may be reduced if patients identified as critically ill and dying have PC consultation in the ED. This may in turn reduce suffering and improve quality of care.1 Based on this study, we recommend education of PC and ED providers with regard to partnering and identification of appropriate patients for PC consultation. Early PC consultation may facilitate efficient patient disposition as well as enhanced communication and decision making. ED providers could use palliative care skills for pain and symptom management, as well as communication techniques for goal clarification and end-of-life discussions. There is tremendous potential for collaborative research in this area, including development of needs assessment and development of a standardized screening tool for PC consultation criteria. The data suggests that PC programs may reach patients appropriate for PC by establishing a partnership with ED personnel. 1. Khatcheressian J, Cassel JB, Lyckholm L Coyne P, Hagenmuller A, Smith T: Improving Palliative and Supportive Care in Cancer Patients. Oncology. 2005;19:1365-1376. Table 1: Medical cases ending in death. Figure 1: Admissions from ED to PCU. Figure 2: Medical cases ending in death. Objectives 1.To describe the relationship between the ED and PC services at a large, urban teaching hospital. 2. Describe the characteristics and outcomes of patients admitted through the ED directly to the PCU. 3. Describe costs and LOS of patients admitted to the ICU and other areas compared with that of patients admitted directly to the PCU. 4. Demonstrate potential need for mutual education and collaboration between PC and ED services. Contact: jbcassel@vcu.edu and lyckholm@vcu.edu V i r g i n i a C o m m o n w e a l t h U n i v e r s i t y






















