Download
1 / 17
170 likes | 199 Views
Learn about the role of psychologists in palliative care, collaboration challenges in different team settings, and solutions for effective interdisciplinary care. Join Dr. Marasco for expert insights.

E N D
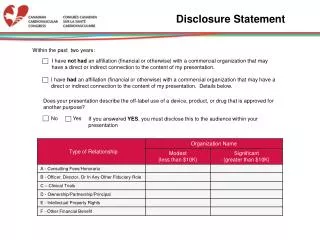
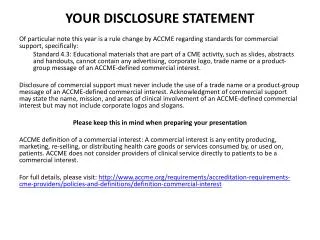
2011 PPEDisclosure Statement2011 PPE DISCLOSURESTATEMENT It is the policy of the Oregon Hospice Association's (OHA) Continuing Medical Education Program to insure balance, independence, objectivity, and scientific rigor in all its educational programs. All faculty participating in any OHA-sponsored programs are expected to disclose to the program audience any real or apparent affiliation(s) that may have a direct bearing on the subject matter of the continuing education program. This pertains to relationships with pharmaceutical companies, biomedical device manufacturers, or other corporations whose products or services are related to the subject matter of the presentation topic. The intent of this policy is not to prevent a speaker from making a presentation. It is merely intended that any relationships should be identified openly so that the listeners may form their own judgments about the presentation with the full disclosure of the facts. Dr. Marasco is the Founder and Director of Transitions Professional Center.
The Role of the Psychologist in Palliative Care and Hospice • Louise E. Marasco, Ph.D. • 9/28/11
What Psychologist? • Traditional Hospice model; physician, nurse, chaplain, social worker. • Examples of when psychologist is consulted (inpt & outpt) • Pt suffers from MH problems less familiar to team • SMI, PTSD, SI, NP Deficits, PD, Substance Dep/Abuse, Gender Reassignment... Compicated Bereavement
Palliative Care & Hospice Psychologist • Skills; Clinical, Assessment, Research, Education • *Assessment * Research*
Palliative Care & Hospice Psychologist • Effective Collaboration • Challenges • A. (Team Level Challenges) Team Type - multidisciplinary, interdisciplinary, transdisciplinary • B. (Team Member Level Challanges) Overlap with other allied health professionals • C. (System Level Challanges) Billing for services 5
Palliative Care & Hospice Psychologist • Effective Collaboration • Improved use of meds, decreased length of hospitalization, decreased medical costs 1 • Failure - poor pt care, unhealthy work environment 7
Effective Collaboration • Team Level Challenges • A. Team Type:MultidisciplinaryInterdisciplinaryTransdisciplinary
Effective Collaboration • Multidisciplinary Teams • Members of different disciplines work together, function independently • Minimal coordination or consultation • Individuals own their tx plan, though often integrate input from others • Hierarchically organized - leadership & decision making not shared • Decision making vertical 1, 2, 3, 4
Effective Collaboration • Interdisciplinary Teams • Providers from different disciplines colloboratively and interdependently plan, implement and evaluate outcomes of care • Division of tasks among team members is based more on pt problems and needs than on role definitions 2 • Decision making and leadership are shared and are flexible 3,4 • Consensus of goals and strategies • Recogntition of shared responsibility, unique competencies, contriubutinos and roles of each ddiscipline and areas of overlapping function 4, 5 9
Effective Collaboration • Transdisciplinary Teams • Professionals from different disciplines who teach, learn, and work together across professional boundaries • Roles & responsibilities are shared, disciplinary lines blurred, few seams b/t members’ functions; “role release” 6
Effective Collaboration • Solutions to risk of functioning as silo • Pursue Regular Communication/Consultation/Collaboration • Phone, email, regular meetings, IDT meetings, videoconferencing • Determine frequency - consider obstacles & solutions
Effective Collaboration • Team Member Level Challenges • B. Overlap with other allied health professionals • Role confusion, unclear expectations, turf issues • Ex: Team member asks another team member to carry out a task... Opportunity to educate team re roles • Highlights: trust, effective communication, the need for educating team members re roles, early clarification among allied health professionals • Tools for strong effective collaborative relationships: make time, practice timely, concrete, non-judgemental feedback
Effective Collaboration • System Level Challenges • C. Billing for services • Billable hours - limited for psychologists • IDT meetings and other collaboration efforts usually not billable • Medicare reimbursesment low
Effective Collaboration • System Level Challenges • Solutions for Psychologists • New Model: Transitions Professional Center • Clinical * Assessment * Research * Education • Training Program: Serve the Community for Minimal Fees ~ Ph.D./PsyD graduate students gain optimal palliative care training • Limited Number of Insured Pts/Provider
Transitions Professional Center, LLC • Clinical: Individual, Couples, Family Therapy • Assessment: Neuropsychological Screens, Integrated Batteries, Capacity Evaluations • Teaching: Graduate Level Training Program, Practicum Level, Post-doctoral Level, Professional Level Educational Series, CE Workshops • Research: Palliative Care, Hospice, EOL, Loss and Bereavement • Interdisciplinary Members ~ Phone Conference, Video Conferencing Capabilities • Consultation Services, Inservices • Home Visits • All Palliative Care, EOL, Bereavement Discipline Networking Opportunities • Events open to the public
Palliative Care & Hospice Psychologist • Conclusion: • PC & H Psychologists - Psychotherapy, Assessment, Research and Education • Effective Collaboration • Team level challanges - Support for Psychologist Functioning as Interdisciplinary Member • Team Member Level Challanges - Role Overlap with Allied Health Providers • System Level Challanges - Present Transitions Professional Center Model
References • Anderson, R., Marasco, L., Kasl-Godley, J., & Kennedy, S., Social Work and Psychologists. In Altilio, T. & Otis-Green, S. (Eds.), Oxford Textbook of Palliative Social Work (pp 425-435). New York, NY: Oxford University Press. • 6. Larson, D.G. (1993). The helper’s journey: Working with people facing grief, loss, and life-threatening illness. Champaign, IL: Rsearch Press. • 7. Larson, E. (1999). The impact of physician-nurs interaction on patient care. Holisitc Nursing Practice, 13(2), 38-46. • 5. Lickiss, J. N., Turner, K. S., & Pollock, M. L. (2004). The interdisciplinary team. In D. Doyle, G. Hanks, N. I. Cherny, & K. Calman (Eds.), Oxford textbook of palliative medicine (3rd ed., pp. 42–46). New York, NY: Oxford University Press. • 2. Zeiss, A. M., & Gallagher-Thompson, D. (2003). Providing interdisciplinary geriatric team care: What does it really take. Clinical Psychology: Science and Practice, 10, 115–119. • 3. Zeiss, A. M., & Steffen, A. M. (1996). Interdisciplinary health care teams: The basic unit of geriatric care. In L. L. Carstensen, B. A. Edelstein, & L. Dornbrand (Eds.), The practical handbook of clinical gerontology (pp. 423–450). Thousand Oaks, CA: Sage Publications. • 4. Zeiss, A. M., & Steffen, A. M. (1998). Interdisciplinary health care teams in geriatrics: An international model. In A. S. Bellack & M. Hersen (Eds.) Comprehensive clinicalpsychology: Clinical geropsychology (Vol. 7, pp. 551–570). New York, NY: Elsevier Science. • 1. Zwarenstein, M., Goldman, J., & Reeves, S. (2009). Interprofessional collaboration: Effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database of Systematic Review, 3. Retrieved from http://www2.cochrane.org/reviews