Download
1 / 50
810 likes | 3.37k Views
Histology of the Breast Rebecca Cook Ph.D. Cancer Biology Department April 21, 2003 Embryonic development Compared to other stages of breast development, fetal development of breast tissue is relatively independent of sex steroid hormones

E N D
Histology of the Breast Rebecca Cook Ph.D. Cancer Biology Department April 21, 2003
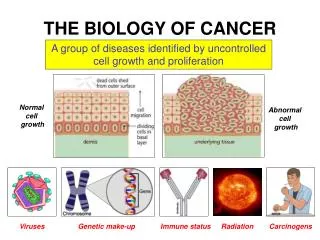
Embryonic development Compared to other stages of breast development, fetal development of breast tissue is relatively independent of sex steroid hormones Week 4--Mammary ridges appear as thickened lines of epidermis that extend from the axilla to the medial thigh. Weeks 5-7--Proliferation of the mammary ridge ectoderm results in primary bud formation which grows down into the dermis. Weeks 10-12--The primary bud branches to form secondary buds. 3 mo.-birth--The buds lengthen and branch. During the last 3 months of gestation the buds canalize to form the lactiferous ducts.
Breast development during puberty • Female breast development is reinitiated to produce the stuctures that will allow for lactation later in life (regulated by steroid and peptide hormones and growth factors). • The male breast remains a rudimentary system of simple ducts within a small amount of fibrocollagenous tissue. • The growth regulatory and differentiation mechanisms involved in development, maintenance, and function of the mammary glands beginning at puberty include systemic, local, cell surface and intracellular controls.
Hormonal regulation and characteristics of breast development at puberty The onset of cyclic production of estrogen and progesterone at puberty leads to the characteristic anatomical and histological changes of mature breasts. Anatomical changes include: 1. Breast enlargement due to an increase in adipose tissue (estrogen-dependent) and breast parenchyma. 2. Full pigmentation of the areola and nipple (dependent on estrogen, progesterone, and pituitary peptide hormones).
Enlarging Pubescent Breast Ducts Adipose tissue Dense CT septa
Branching ductal tree of prepubescent breast Convergence of major ducts Early formation of terminal ductal lobular units (TDLU) Whole mount preparation
Histological changes occurring in the breast at puberty • Estrogen, progesterone, growth hormone and prolactin are the major hormones involved in breast development during puberty. Histological changes occurring in response to these hormones include: • Ductal elongation and thickening of the ductal epithelium (Progesterone is not required for ductal growth during puberty) • Increased connective tissue density surrounding the ducts • Formation of Terminal ductal lobular units (TDLU, functional units of the breast) which is dependent on both estrogen and progesterone. • TDLU are also referred to as lobulo-alveoli, acini, and lobules.
Lobules 1-2 mm Ducts Young adult breast
Appearance of ducts and alveoli in the immature breast Ducts and alveoli consist of 2 cell layers: 1. Basally localized myoepithelial cells that are flattened and have pale cytoplasm 2. Luminal cuboidal epithelial cells In comparison to alveolar epithelial cells, ductal epithelial cells contain few mitochondria and sparse ER Changes occurring in the ducts and alveoli during the menstrual cycle: 1. Early in the cycle lumens of the ducts aren’t clearly evident 2. Later in the cycle ductal lumens become apparent and may contain eosinophilic secretion.
Early pubescent breast TDLU Adipose tissue Duct Dense CT
Characteristics of mature breasts • Breast size ranges from <30g to >500g. Size varies with body weight since breast is a major repository of adipose tissue. • 15-25 lobes, each empties into terminal duct at nipple • Dense CT septa divide lobes • Each lobe is divided into many TDLU
Nipple • Ectodermally derived • 15-25 milk ducts enter the base of the nipple where they dilate to form the milk sinuses • Milk sinuses terminate into cone shaped ampullae (milk repositories) below the nipple surface • Ampullae of non-lactating women are plugged with keratin to prevent infection of the breast through the nipple • Nipple erection and emptying of the milk sinuses is controlled by circular and longitudinal smooth muscle fibers, collagen and elastic CT • Areola contains sebaceous glands of Montgomery whose secretions are thought to protect the areola and nipple during suckling
Non-lactating nipple and areola Keratin Plugs
Higher magnification of a lobule BM surrounds each alveolus Interlobular Dense CT IntralobularLoose CT
Alveolar cell types in the mature breast Alveolar epithelium is specialized into type A, B and myoepithelial cells. Type A: Luminally located, columnar cells, basophilic because they are rich in ribosomes. Synthesize and secrete milk components. Type B: Thought to be the precursors of Type A and myoepithelial cells. Basally located with clear cytoplasm and round nuclei. Myoepithelial cells: Basal cells with dense nuclei that are in close contact with the luminal secretory cells. Glycogen production gives cells a clear cytoplasm when stained with H&E. Contain myofibrils that allow the cells to contract to help in milk secretion.
Myoepithelial cells Loose CT Cell types found in alveoli Columnar secretory cells BM
IHC staining of actin demonstrates the presence of myoepithelial cells
The appearance of secretory epithelial cells varies with duct and lobule size Smaller ducts/lobules Larger ducts/lobules
Myoepithelial cell lipid droplets Myoepithelial cell Secretory cells EM of a single lobular unit Lumen
Normal variations in the breast associated with hormonal changes during the menstrual cycle • Cyclic progesterone and estrogen associated with a full ovulatory cycle drive development of TDLU and connective tissue growth into a woman’s 30s. In the absence of pregnancy, apoptosis of the expanded epithelium within the TDLU occurs. • Differentiation effects of progesterone: • Myoepithelial cells accumulate glycogen • Epithelial cells develop more prominent nucleoli and secretion • Stromal changes occur with an increase in intra and inter-lobular edema • Several anovulatory menstrual cycles can lead to increased accumulation of secretions, edema, and mononuclear cell infiltrates resulting in transiently cystic structures.
Breast development during early pregnancy • Extensive epithelial cell proliferation and expansion of lobular alveolar/TDLU at the expense of the adipose and connective tissue. • Requires estrogen, progesterone, prolactin, growth hormone, and insulin. • Colostrum secretion begins around the 3rd month of pregnancy.
Breast development during the 2nd trimester of pregnancy • Rate of epithelial proliferation begins to decline. • Alveoli epithelium appears monolayered and flattened while ductal epithelium maintains appearance of 2 cell layers. • Alveolar epithelium begins to differentiate and assume a presecretory function. • Requires prolactin, human placental lactogen, growth hormone, insulin and glucocorticoid. • Milk proteins and lipids are actively synthesized, but only small amounts are released. • Prolactin regulates secretion and its levels increase throughout pregnancy. Luteal and placental hormones (progesterone) antagonize prolactin activity preventing lactation until parturition.
Colostrum secretion increases during the later stages of pregnancy
Eosinophilic Milk proteins Lipid vacuoles Higher magnification of lactating breast Epithelium appears squamous
Both apocrine and merocrine secretion patterns are involved in milk secretion Merocrine secretion: Lactose and proteins Apocrine secretion: Lipids
Hormonal control of lactation • Milk secretion is controlled by prolactin, glucocorticoid, growth hormone, insulin, and thyroid hormone. • Prior to parturition the pro-secretory effect of prolactin is antagonized, mainly by progesterone. • Suckling maintains continued milk production by releasing prolactin and adrenocorticotropic hormone. • Suckling also stimulates oxytocin release from the posterior pituitary which induces myoepithelial cell contraction and ejection of milk from the alveoli into the ductal system.
The composition of milk varies during lactation • Colostrum is the first secretion following parturition: • Antibody rich, especially in IgA-produced by plasma cells in the loose CT around the alveoli. Confers passive immunity to infant. • Typically richer in protein and much lower in fat than mature milk. • Available for the first few days after birth and is then replaced by mature milk. • Mature milk: • Contains water, Na+ K+ Cl- Ca2+ and PO43+, protein (lactalbumin and casein), carbohydrates (lactose), lipids (mainly triglycerides), vitamins and antibodies (mainly IgA). • Approximately 1-2 ml of milk/g of breast tissue per day is produced.
Cessation of lactation causes glandular involution • Involution is the process by which in the absence of lactation, the alveoli are reduced in number and size due to apoptosis of the expanded secretory epithelium. • Remaining alveolar epithelium returns to a non-secretory 2 cell layered epithelium. • Breast returns to a more ductular system characteristic of the inactive mature breast. • New connective and adipose tissues form between the involuted mammary alveolar structures. • Complete regression of the glands takes about 3 months.
Post-menopausal breast • Involution is dependent upon declining levels of estrogen and progesterone. Little else is known about which factors control this process. • In contrast to post-lactational involution during which the number and size of alveoli is reduced, post-menopausal breast involution is characterized by regression of the parenchymal TDLU. • Deposition of adipose tissue and connective tissue increases. • At completion of involution only small islands of the ductal system remain embedded in dense fibrous connective tissue. • Normal histology of postmenopausal breast varies.
Atrophic lobules Secretion Higher magnification of branching ductal tree in aging breast
Appearance of the ductal tree and TDLU in a 59 year old woman Distended ductal tree Moderately atrophic lobules
Lobules 1-2 mm Ducts Young adult breast
Normal lobule from non-cancerous breast of an 83 year old woman Fewer lobules Increased density of intralobular CT
Higher magnification of a lobule BM surrounds each alveolus Interlobular Dense CT IntralobularLoose CT