Download
1 / 22
220 likes | 574 Views
Patch Me if You Can! What Internists Need to Know About Allergic Contact Dermatitis. Mark H. Lowitt, MD Clinical Associate Professor of Dermatology University of Maryland School of Medicine Private Practice, Greater Baltimore Medical Center. Contact Dermatitis. Cases

E N D
Patch Me if You Can!What Internists Need to Know About Allergic Contact Dermatitis Mark H. Lowitt, MD Clinical Associate Professor of Dermatology University of Maryland School of Medicine Private Practice, Greater Baltimore Medical Center
Contact Dermatitis • Cases • Clinical Features of Allergic Contact Dermatitis • Mechanisms of Allergic Contact Dermatitis • Patch Testing
Case 1 51 y/o F • Phlebotomist • Itchy and painful fingers and hands, worsening over years • Not seasonal • What’s the diagnosis? • What’s the cause?
Case 2 • Same photo 73 y/o F • Severe eyelid pain and itch worsening over weeks • What’s the diagnosis? • What’s the cause?
Case 3 40 y/o M Auto mechanic for 20 years Similar eruption on feet • What’s the diagnosis? • What’s the cause?
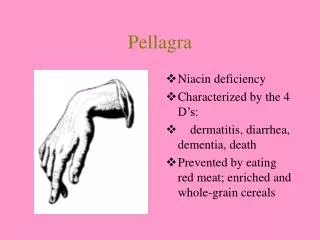
Erythema • Edema • Vesiculation • Scaling • Lichenification • Well defined edges and Straight lines • Pruritus • History: The more you treat, the worse it gets
What’s new in contact dermatitis? • What makes a good contact allergen? • Low molecular weight • Lipophilic • Able to form covalent bonds with nucleophilic residues on amino acid side chains • Sensitizing potential may be related to chemical reactivity toward a few specific amino acids involve in sensitization • Esp. cysteine residues
North American Tray • Metals: Nickel, Gold, Cobalt, Copper • Fragrances: Fragrance mix, Balsam of Peru, Isoeugenol, Lyral • Preservatives: Quaternium-15, Paraben mix, Formaldehyde, Kathon CG, Propylene glycol, Thimerosol • Medications: Neomycin, Bacitracin, Tixocortol-21-pivalate, Budesonide • Dyes: P-phenylenediamine, Disperse blue • Rubber products: Mercaptobenzathiazole, Carba mix, thiuram mix, mixed dialkyl thiourea • Other: Benzocaine, Colophony, ethyl acrylate
Hand Dermatitis • Allergic Contact Dermatitis • Irritant Contact Dermatitis • Dyshidrotic Eczema • Palmar psoriasis • Tinea Manum • Mycosis fungoides
Hand Dermatitis • Patch test positive for Quaternium-15 • Common preservative
Chronic Hand Dermatitis • Major Occupational Health Problem • 40% of all Occupational Health Claims are from skin • 90% of these are Dermatitis • 65% are Irritant Contact • 35% are Allergic Contact • THEREFORE, 12% OF ALL WORKMAN’S COMP CLAIMS ARE DUE TO ALLERGIC CONTACT DERMATITIS
Allergic Contact Dermatitis of the Hands • 22,035 patients patch tested between 1994 and 2004 • 6953 had hand involvement • 959 with a solitary dx of ACD • Quaternium-15 17% • Formaldehyde 13% • Nickel 12% • Fragrance Mix 11% • Thiuram Mix 10%
Eyelid Dermatitis • Differential Diagnosis • Contact dermatitis • Atopic dermatitis • Dermatomyositis Atopic dermatitis Dermatomyositis (heliotrope rash)
Patch testing: • Positive for Gold sodiumthiosulfate • May be 10% of positive patch tests • More common in women • 8% of gold + pts have eyelid dermatitis • Clinical picture can be confusing due to presence of nickel in gold alloys
Eyelid Dermatitis • Most common causes of eyelid allergic contact dermatitis: • Gold 22% • Fragrance mix 19% • Balsam of Peru 17% • Nickel 16% • Neomycin 9%
Treatment with topical cortisones initially help, but then the condition worsens Tinea manum (dermatophyte infection)
Patch test positive for Budesonide • Cross reacts with triamcinolone, fluocinonide, fluocinolone, desonide, budesonide • Corticosteroids were the American Contact Dermatitis Society 2005 “Allergen of the Year”
Corticosteroid allergy • Class A Hydrocortisone and tixocortol type • Cortisone, hydrocortisone, methylprednisolone, prednisolone • Class B Triamcinolone acetate type • Triamcinolone, halcinonide, flucinonide, fluocinolone, desonde, budesonide, amcinonide • Class C Bethamethasone type • Betamethasone, dexamethasone, flucortolone • Class D Hydrocortisone-17-butyrate and clobetasol 17- butyrate
Allergic Contact Dermatitis: Review • Have a high index of suspicion for ACD • Angulated lesions with straight edges and unusual shape • A refractory dermatitis • However, keep your mind open: not all dermatitis is allergic
Allergic Contact Dermatitis: Review • Patch testing can help to identify the allergen • Hand dermatitis most often caused by quaternium-15 • Eyelid dermatitis most often caused by gold • In pts not getting better, consider contact dermatitis to topical steroids
Interested in patch testing? www.contactderm.org American Contact Dermatitis Society (ACDS) www.dormer.com Dormer Labs (Canada) patch test materials www.allergEAZE.com patch test materials