Download
1 / 34
2.74k likes | 17.63k Views
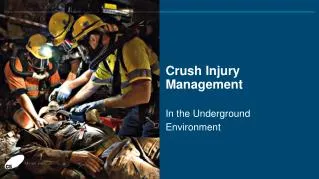
CRUSH INJURIES Crush Injury Compression of body parts causing localized muscle and nerve damage. Frequent injury seen in both natural (earthquakes, tornadoes, etc.) and man-made (bombings, industrial accidents, etc.) disasters. ©2010 Trauma and Disaster Institute Crush Injuries

E N D
CRUSH INJURIES Crush Injuries
Crush Injury • Compression of body parts causing localized muscle and nerve damage. • Frequent injury seen in both natural (earthquakes, tornadoes, etc.) and man-made (bombings, industrial accidents, etc.) disasters. ©2010 Trauma and Disaster Institute Crush Injuries
Incidence • Lower extremities = 74% • Upper Extremities = 10% • Trunk = 9% Crush injury with amputation, El Salvador earthquake (1987) Crush Injuries
Crush Syndrome • “Crush syndrome” first recorded in bombing of London during WWII. • 5 people who were crushed presented in shock with swollen extremities and dark urine. • All later died from renal failure. Crush Injuries
Crush Syndrome • Localized crush injury with systemic manifestations • Systemic effects caused by traumatic rhabdomyolysis (muscle breakdown) and the release of toxic muscle cell components and electrolytes into the circulatory system Crush Injuries
Crush injury of pelvis with secondary crush syndrome Crush Syndrome Common in Earthquakes Crush Injuries
Earthquakes • Incidence of crush injury is 2-15% (historical data). • ~ 50% develop acute renal failure. • ~ 50% of those with acute renal failure need dialysis. • > 50% of casualties require fasciotomies. Crush Injuries
Components of Crush Syndrome • Local tissue injury • Organ dysfunction • Metabolic abnormalities Crush Injuries
Metabolic Abnormalities • Acidosis (low blood pH levels) • Hyperkalemia (high potassium levels) • Hypocalcemia (low calcium levels) Crush Injuries
Definitive Management of Crush Syndrome Crush Injuries
Key Principles: • ADEQUATE FLUID RESUSCITATION is critical in treating victims of crush injury. • Ideal resuscitation fluid: Normal Saline Crush Injuries
Secondary Treatment Modalities • Bicarbonate • Mannitol (no proven benefits but no significant deleterious effects) Crush Injuries
Goals of Fluid Therapy: • Prevent tubular precipitation of myoglobin • Decrease risk of hyperkalemia • Correct acidemia Crush Injuries
Prehospital Considerations in the Management of Victims with Crush Injuries Crush Injuries
TREATMENT ALERT! • Pretreat casualties with prolonged crush (> 4 hrs), as well as those with abnormal neurological or vascular exams • 1-2 liters Normal Saline BEFORE releasing crush object whenever possible! Crush Injuries
TREATMENT ALERT! • If not possible to pretreat, consider applying tourniquet to crushed limbs and maintain until IV fluid administration is initiated. Combat Application Tourniquet (CAT) Crush Injuries
Key Principle: • Risk of acute deterioration and death with sudden release of pressure on the involved extremity (REPERFUSION SYNDROME). Crush Injuries
Reperfusion Syndrome • Acute hypovolemia • Metabolic abnormalities Crush Injuries
TREATMENT ALERT! • Metabolic abnormalities • Acidosis: IV sodium bicarbonate to prevent myoglobin deposits in kidneys • Hyperkalemia: Calcium, sodium bicarbonate, insulin/D5W • Hypocalcemia: Calcium Crush Injuries
TREATMENT ALERT! • Delays of hydration for longer than 12 hours increase the incidence of renal failure. Crush Injuries
Late Treatment: Dialysis Crush Injuries
Compartment Syndrome • Following traumatic injury, the muscles within a compartment can swell, causing irreversible damage to nerves, vascular structures, and muscles. • Compartment syndrome is a medical emergency. Crush Injuries
Compartment Syndrome • Consider the possibility of a compartment syndrome in all patients with significant crush injury. • Compartment syndrome reported with trapping times less than 1 hour. • Fracture not mandatory for compartment syndrome to develop. Crush Injuries
RISK ALERT! • Peripheral pulses may be present in the early stages of limb ischemia. Crush Injuries
Field Observation… • The cardinal symptom of compartment syndrome is pain out of proportion to apparent injuries. Crush Injuries
Upper Extremity Compartment Syndrome • Forearm and hand are at highest risk. Crush Injuries
Lower Extremity Compartment Syndrome • Anterior and lateral compartments of the lower leg (calf) are at highest risk. Crush Injuries
Fasciotomy • The decision to undertake fasciotomy should be made based on a high index of suspicion of a compartment syndrome in patients with complex extremity injuries. • Err on the side of early fasciotomy. Crush Injuries
Lower Extremity Fasciotomies Crush Injuries
Early Mortality in Crush Syndrome • Hypovolemia • Hyperkalemia Crush Injuries
Late Mortality in Crush Syndrome • Sepsis • Multiple Organ Failure Crush Injuries
Factors Impacting Mortality and Morbidity: • Severity of the crush injury • Timing of treatment • Initial treatment provided to the victim Crush Injuries
Questions… Crush Injuries