Download
1 / 45
450 likes | 1.1k Views
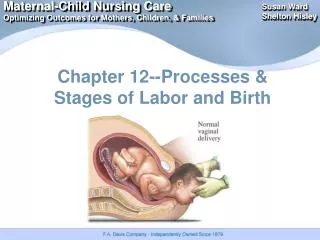
Stages of labor. Chapter 16, 17, 18, 19. Stages of Labor. First Stage Latent phase Active phase Transition phase Second Stage Third Stage Fourth Stage. First stage of labor :(Stage of Dialtion)

E N D
Stages of labor Chapter 16, 17, 18, 19
Stages of Labor • First Stage • Latent phase • Active phase • Transition phase • Second Stage • Third Stage • Fourth Stage
First stage of labor:(Stage of Dialtion) • It begins with the onset of true laborcontractions and ends with complete dilation (10cm) and effacement (100%) of the cervix. • It is the longest stage for both nulliparous and parous women. • Ithas three phases: latent (early), active, andtransition.
1. Latent phase: • Lasts from the beginning of labor until about 3cm of cervical dilation. • The woman is usually sociable and excited during this phase of labor. • Uterine contraction initially mild and infrequent progress to moderate strength every 5 min.
2. Active phase: • The cervix dilates from 4 to 7 cm • Effacement is completed • The fetus descends to the pelvis • Internal rotation begins • Increase discomforts • The woman becomes more anxious and feel helpless • Serious inward focus • Uterine contraction every 2-5 minute
3. Transition phase: - Short but intensephase • The cervix dilate from 8 to 10cm • The fetus descends further into the pelvis • Bloody show increase • Strong contractions • The woman may have the urge to push down • Leg tremors nausea and vomiting are common • The woman is irritableand lose control • Contraction every 1.5-2minute
Second stage of labor (expulsion): • Begins with complete dilation (10cm) and fulleffacement(100%) end with the birth of the baby. • involuntary pushing response • The mother may said that she needs to have a bowel movement or the baby is coming • Crowning of the fetal head • Feeling of stretching or splitting sensation • Contractions are strong • Woman exerts intense effort to push her baby • May appear sleepy between contraction • The word “labor” describe this phase • Feels tremendous relief and excitement as the second stage ends with the birth of baby
Second stage of labor(Expulsion) • Crowning of the fetal head
Third stage of labor (placental) • Begins with the birth of the baby and ends withthe expulsion of the placenta • Length 5-10 min up to 30 min • Four Signs suggest placental separation: • 1.Spherical shape of uterus • 2.The uterus rises upward in the abdomen • 3.The cord descends further from the vagina • 4.a gush of blood appears as blood trapped behind placenta is released
The uterus must contract firmly and remain contracted after placenta is expelled to compress open vessels • During this stage pain results from uterine contractions and brief stretching of cervix as placenta passes through it
Fourth stage of labor (physical recovery): • It lasts from the delivery of the placenta through the first 1 to 4 hours after birth • The uterus at or below the level of umbilicus ,firm contracted and rounded mass about 10 to 15cm in diameter • Lochia is rubra • Women may have chill lasts for 20 minutes, warm blanket or hot drink may be helpful
After pains or birth trauma are the main causes of discomforts in this stage • Ice packs on perineum decrease discomfort and limit hematoma formation • After pains are more intense in multiparous or in women who breast feed, in women who have uterine over distention( large baby) and full bladder or clot that remain in uterus • The woman is exhausted and need rest • This stage is the ideal time for bonding and to start breast feeding
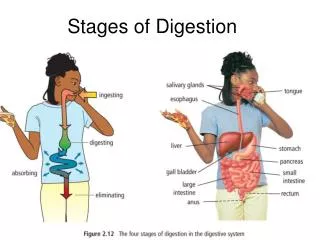
Nursing care during labor and birth • Assessment on admission • Focused assessment • 1. Fetal assessment • Gestational age of the fetus • Leopold’s maneuver • Fetal movement and FHR • Status of membrane( color ,odor and clarity of fluid) • 2. Maternal assessment (vital signs) especially for infection or hypertension
Data base assessment • Reason for coming to hospital • Prenatal care • EDD • # of pregnancies term and abortion • Allergies • Last time of food intake • Medical surgical and pregnancy history • Recent illness and treatment • Medication, drug smoking and alcohol • Mother subjective evaluation of labor • Birth plan, pain management method and support person
2.Fetal assessment • Presentation ,position and FHR • Time of rupture membrane and characteristics ofamniotic fluids • 3.Determine labor status • Assess contraction • Cervix dilitation and effacement, station ,presentation and position • Membrane status
4. Physical exame(brief) • 5. Laboratory data • Hematocrite and blood group and CBC • Blood glucose levels • Blood type and RH factor • Midstream urine(protein and glucose) • Syphilis ,hepatitis and HIV • 6.IV access • Continuous infusion prevent dehydration • Isotonic electrolyte is preferable • Glucose is avoided
Assessment after admission • 1.Fetal assessment • FHR electronic or Doppler • Amniotic fluid AROM OR SROM • Assess FHR at least one min after rupture of membrane • Record the time of rupture,FHR and character of fluid cloudy, yellow or foul odor suggest infection • Green color suggest meconium passage (transient hypoxia) • Amount more than 1000ml is large, between 500-1000 is moderate and scant if only trickle barely enough to detect
A typical CTG output for a woman not in labour. A: Fetal heartbeat; B: Indicator showing movements felt by mother (caused by pressing a button); C: Fetal movement; D: Uterine contractions
2. Maternal assessment • Vital signs( hyper or hypotension , increased pulse increased resp. increased temp are all abnormal • Contraction • Progress of labor , vaginal exam should be limited to prevent infection • Intake and output ,check for bladder fullness every 2 hour • LOOK AT THE MOTHER’S PERINIUM FOR CROWNING OF FETAL HEAD IF SHE EXPERIENCE A NEED TO DEFECATE • Mother response to labor
Nursing care for woman in true labor • 1. Fetal oxygenation • Assessment of fetal well being include: FHR,contraction,aminiotic fluid and vital signs • Intervention • 1.promote placental function( position rather thansupine) • 2. observe for condition associated with fetal compromise
Vena Caval Syndrome (Supine Hypotensive Syndrome) Fig. 13-4a
Conditions Associated with Fetal Compromise • Fetal heart rate outside the normal range • Little or no variability in heart rate • Persistent slowing of heart rate after contractions • Meconium-stained amniotic fluid • Cloudy, yellowish, or foul odor to amniotic fluid • Contractions longer than 90 seconds • Incomplete uterine relaxation, intervals between contractions shorter than 60 seconds • Maternal hypotension • Maternal hypertension • Maternal fever
2. Discomfort • Intervention • 1. providing comfort measures • Lightening: soft indirect lighting is soothing • Temperature; Cool damp cloths on woman's face and neck promote comfort, an electric fan circulate air in the room is appropriate (should be turned off before delivery of the newborn) • Cleanliness: change gown and linen when needed
Mouth care: ice chips and hard candy reduce discomfort of dry mouth, avoid excessive sugar and if oral intake is contraindicated brushing teeth or rinsingmouth • Bladder emptying; Remined woman to empty bladder at least every 2 hours, catheterization is often needed • Positioning: use any comfortable position but avoid supine • Water( shower, tub, pool): enhance relaxation . Nipple stimulation by water current release oxytocin and make contraction more productive
2. Teaching • First stage • Pushing in response only to her spontaneous urge • Pushing without full dilitation leads to cervix become lacerated and edematous and progress is blocked • Second stage • Laboring down • Position( curve body around uterus in C shape)
3. Teaching cont. • Second stage • Laboring down: researchers recognized that a second stage longer than 2 hours is safe if the mother and fetus show no signs of compromise. • Women push most effectively when they feel the reflex urge to do so. • Discourage Closed-glottis pushing or the Valsalva maneuver because it can reduce maternal cardiac output reduce fetal oxygenation. • Position: the mother may push in any preferable position. Change position. curve body around uterus in C shape with her chin on her chest. For most effectiveness, teach her to pull on her knees, hand- holds, or a squatting bar while pushing.
3. Teaching cont. • Breathing pattern: • discourage holding breath more than 4 second per push • discourage pushing more than four times per contraction. • Deep breath helps her relax at the end of contraction. • Women may grunt or groan (أنين) when pushing reassure her that this is normal. • Provide encouragement • Giving of self:the nurse caring presence is crucial. Gentle coaching, encouragement improve laboring woman confidence in her own body to give birth. • Pharmacologic management and support and care • Caring for the birth partner : woman’s support person
3. Preventing injury assessment ; observe mother’s perineum to determine when to make final preparation Final preparation for primipara is done when crowning reach a diameter of 3-4cm but in multipara when cervix is fully dilated
Intervention • 1. transfer to delivery room • 2. positioning of birth • 3. observing perineum • Nursing care during Birth • 1.Preparation of table • 2.Perineal cleansing preparation • 3.Initial care and assessment of newborn • 4.Administration of medication such as oxytocin to control blood loss • 5.Use universal precaution
Responsibilities after birth • Care of infant • 1. maintain cardiopulmonary function • prepare neonatal resuscitation equipment • Assess Apgar score • Suctioning of secretion • 2. supporting thermoregulation • dry infant • place under radiant warmer • Skin to skin contact
InRev1 The Apgar Scale Score 0 1 2 Characteristic Heart rate Efforts to breathe Muscle tone Skin color Reflex irritability Absent Absent Flaccid,limp Body pale or blue No response Less than 100 beats per minute Slow, irregular Weak, inactive Body pink, extremities blue Frown, grimace More that 100 beats per minute Good; baby is crying Strong, active motion Body and extremities pink Vigorous crying, coughing, sneezing
3. Identifying the infant • Identifying band • Care of the mother • 1. observing for hemorrhage • Vs,fundus,lochia,bladder • Vital signs : assess temp. in recovery and before transfer to postpartum ward • Assess other vital signs every 15 min for first hour and 30 min in the next hour
Fundus should be firm midline and at or below umbilicus .If not firm massage and encourage mother to breast feeding • Bladder: full bladder is suspected when fundus is above umbilicus and or displaced to one side usually the right • The first two or three voiding must be at least 300-400ml each voiding • Lochia is rubra, small clot is okay but large clot is abnormal • Saturation of one pad within the first hour is the maximum normal lochia flow
2. Relieving discomfort • ice backs, analgesics , warmth • Ice packs: to reduce edema and limit hematoma formation • Analgesics:after pain and perineal pain may relieved by mild analgesics. Regular urination reduce after pain because uterus contract effectively • Warmth warm blanket is soothing and shorten the chills that is common afterbirth3.promoting early family attachment • :
Leopold's Maneuvers (1 of 4) Unn Fig. 17-1 Procedure 17-1
Leopold's Maneuvers (3 of 4) Unn Fig. 17-3 Procedure 17-1