Download
1 / 72
730 likes | 970 Views
MNT for the CKD Patient Complicated by a Pressure Ulcer. Stephanie Ruel Sodexo/St. Joseph’s Medical Center. Abstract. Controversy of recommendations Studies: Inconclusive or inadequate. Introduction. Anatomy and Physiology Etiology and pathology Medical management

E N D
MNT for the CKD Patient Complicated by a Pressure Ulcer Stephanie Ruel Sodexo/St. Joseph’s Medical Center
Abstract • Controversy of recommendations • Studies: Inconclusive or inadequate
Introduction • Anatomy and Physiology • Etiology and pathology • Medical management • Medical Nutrition Therapy • The Patient • Conclusion • Future studies • Recommendations
Anatomy & Physiology of the Kidneys Functions • Metabolic waste removal • Electrolyte balance • Fluid balance • Blood pressure control • pH regulation • Plasma volume and osmolality • Glucose homeostasis • Hormone secretion (erythropoietin) • Carnitine synthesis
Anatomy • Afferent arteriole • Glomerulus • Bowmans’s capsule • Proximal tubule • Efferent arteriole • Peritubular capillaries • Renal vein Proximal tubule
Physiology: Electrolyte Balance • Glomerulus: Selective permeability • Ultrafiltrate • Selective resportion and excretion
Physiology: Electrolyte Balance TubuleEfferent arteriole = fluid homeostasis Electrolytes
Physiology: Fluid Balance Two main systems: • Vasopressin • Renin-angiotensin aldosterone system (RAAS)
Vasopressin ↑Blood osmolality or ↓blood pressure Hypothalamus Pituitary gland Kidney ↑blood pressure ↓blood osmolality Vasopressin
Renin-Angiotensin Aldosterone System ↓blood pressure Angiotensinogen Kidney Angiotensin I Angiotensin II Adrenal Aldosterone ↑blood pressure RAAS Renin Lungs
Etiology& Pathology • Diabetes • Hypertension • Family history • Ethnicity • Autoimmune disease • Infection • Severe dehydration • Acute renal failure (ARF)
Diabetic Nephropathy 44% of new CKD diagnoses caused by diabetes
Diabetic NephropathyGlomerular Anatomy mesangium
Hyperglycemia ↑blood glucose afferent arteriole dilation altered hemodynamic regulation ↑blood flow to glomerulus Hypertrophy damage to podocytes Hyperfiltration and mesangial cells Hyperperfusion altered permeability of glomerulus = PROTEINURIA
Proteinuria Inflammatory mediators Proinflammatory cytokines Oxidative stress Inflammation Fibrosis Glomerulosclerosis Kimmelstiel-Wilson lesions
Hypertension Definition • Hypertension: Systolic >140mm Hg or Diastolic >90mm Hg • Prehypertension: 121/81mm Hg – 139/89mm Hg • Normal blood pressure: <120/80mm Hg
Hypertension • Cause and effect • Blood vessel remodeling • Inflammation • Oxidative stress • Arteriosclerosis
Hyaline Arteriosclerosis • Endothelial lesions in blood vessels caused by buildup of hyaline • Decreased action of smooth muscle cells • Inhibited autoregulation • Ischemic tubulointerstitial injury
Dietary Protein Studies – Impact of protein restriction and blood pressure control on progression of CKD: Modification of Diet in Renal Disease (MDRD) study Northern Italian Cooperative Study Group Multiple studies with smaller sample size; data from mid-1980’s to mid-1990’s INCONCLUSIVE, INSIGNIFICANT
Diagnosis Irreversible loss of kidney function with decreased glomerular filtration rate (GFR) and/or evidence of kidney damage that persists >3 months, progressive in nature.
Antihypertensive Therapy • Hypertension: 80-85% • Angiotensin Receptor Blockers (ARBs) • Angiotensin Converting Enzyme (ACE) Inhibitors • Diuretics
Blood Pressure Control/RAAS • Albuminuria >300mg and all diabetic CKD (without hypertension) • ARBs • ACE Inhibitors • Albuminuria <30mg and BP >140/90mm Hg • Target BP <140/90mm Hg • Albuminuria >30mg, BP >130/80mm Hg • Target BP <130/80mm Hg
Improving Cardiovascular Health • Highest risk category for development of cardiovascular disease (CVD) • CVD as cause of death before end-stage renal disease (ESRD) and dialysis • Statins
Glycemic Control • Target HbA1C ~7.0% • Hypoglycemia risk • Medication and lifestyle modification
Overview of Additional Complications • Metabolic Bone Disease • Parathyroid hormone (PTH) • Calcium • Phosphorus • Potassium • Metabolic acidosis • Anemia
Non-pharmacological Interventions • Smoking cessation • Physical activity • Weight management • Functional capacity
New Medication and Treatment • Allopurinol • Avosentan • Mesenchymal stem cells
Renal Replacement Therapy • GFR <10ml/min/1.73m2 • Symptoms: • Electrolyte abnormalities • Acid-base disturbance • Uncontrolled BP and fluid balance • Uremia • Cognitive impairment • Decline in nutritional status • Dialysis
Renal Transplant • Treatment of choice • Earlier decision: • GFR <20ml/min/1.73m2 • Irreversible progression for 6-12 months • Impact: • Reduction of dietary restrictions • Delays or eliminates need for dialysis • Medications to prevent rejection = ↓immunity
Anatomy & Physiology of the Integumentary System Functions: • Conduct sensory data to the brain via nerve endings located in the skin • Protect the body • Regulate body temperature • Synthesize vitamin D • Store energy and water
Development of Pressure Ulcers Injury to the skin and/or underlying tissue as a result of pressure, friction, shear, or ischemia Risk factors: Immobility Poor perfusion of blood supply Moisture Anemia Age Nutrition status 10-18%
Inflammasome Activity • Inflammasomes in kertinocytes • Activation of inflammatory cytokines • Danger signals and wound healing • Youth vs. Aging
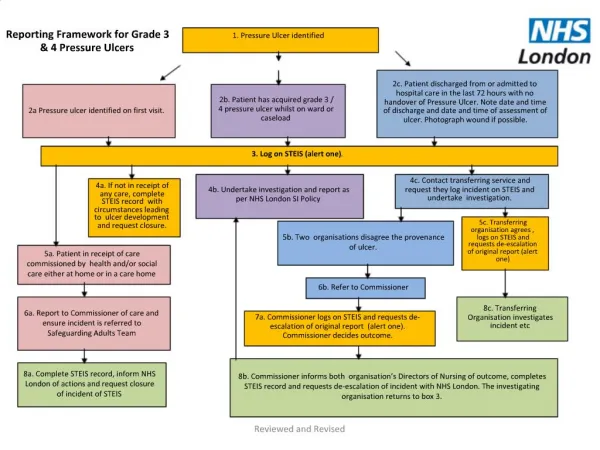
Prevention & Care • Risk assessment (Braden Scale score) • Proper positioning and rotation • Support surfaces • Pain management • Infection management • Wound cleansing • Debridement • Dressings • Biophysical agents
Nutrition Care Process Assessment Diagnosis Intervention Monitoring Evaluation
Assessment • Multidisciplinary • Anthropometrics • Medical and social histories • Medications • Analysis of laboratory values
Nutrition Assessment for CKD • Diet and diet history • Nutrition status • Comorbid conditions • Lab values of BUN, potassium, phosphorus, albumin, urinalysis • Assess for education needs
MNT for Hypertension and Diabetes Diabetes: glycemic control through consistent-carbohydrate diabetes meal planning Hypertension:
The Role of Dietary Protein • Dietary protein restriction did not significantly slow progression • Dietary restrictions and nutrition status • BP control was more effective in reducing proteinuria than modifications in dietary protein intake