Download
1 / 13
130 likes | 409 Views
Long-acting and intermediate acting insulin analogues These slides should be used in conjunction with the accompanying notes. Options for local implementation NPC. Key therapeutic topics – Medicines management options for local implementation. Second update July 2011.

E N D
Long-acting and intermediate actinginsulin analoguesThese slides should be used in conjunction with the accompanying notes
Options for local implementationNPC. Key therapeutic topics – Medicines management options for local implementation. Second update July 2011 • Review and, where appropriate, revise prescribing of long-acting insulin analogues in type 2 diabetes mellitus to ensure that it is in line with NICE guidance
Key questions • What do NICE say about the use of insulins in type 2 diabetes? • What do NICE say about the use of long-acting insulin analogues in type 2 diabetes? • How are we doing with prescribing?
Type 2 diabetes management is multifactorial Smoking Control blood pressure Education Lifestyle Control blood glucose Individualised care of patients: based on evidence for each intervention Statin Aspirin Metformin These slides should be used in conjunction with the accompanying notes
Drug treatment for blood glucose control Based on NICE Clinical Guideline 87; May 2009 and MeReC Bulletin Vol. 21, No. 5, June 2011 Third-line HbA1c ≥ 7.5% (59mmol/mol) or other higher level Safety and tolerability issues Polypharmacy Second-line HbA1c ≥ 6.5% (48mmol/mol) or other higher level First-line *other options are available in specific circumstances
What do NICE say about the use of insulinsin type 2 diabetes?NICE Clinical Guideline 87; May 2009 • Usual third-line option is to initiate insulin therapy in addition to metformin and a sulfonylurea • ‘for a person on dual therapy who is markedly hyperglycaemic, insulin therapy should be considered in preference to adding other drugs to control blood glucose unless there is strong justification not to’ • Intermediate acting human isophane insulin (also called human NPH insulin) remains preferred basal insulin, taken at bedtime or twice-daily according to need • alternatives may be considered in particular patient circumstances
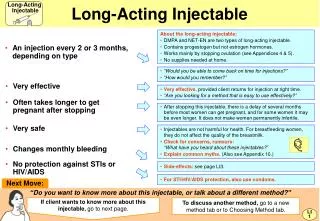
What do NICE say about the use of long-acting insulin analogues in type 2 diabetes? NICE Clinical Guideline 87; May 2009 • Long-acting insulin analogues may be considered as an alternative to human NPH insulin if: • the patient needs assistance from a carer or health professional to inject insulin, and use of a long-acting insulin analogue would reduce the frequency of injections from twice to once daily • the patient’s lifestyle is restricted by recurrent symptomatic hypoglycaemic episodes • the patient would otherwise need twice-daily NPH insulin injections in combination with oral glucose-lowering drugs • the patient cannot use the device to inject NPH insulin
What is the evidence for long-acting insulin analogues in type 2 diabetes?NICE (Short) Clinical Guideline 87; May 2009 No data on long-term complications of diabetes No long-term safety data Compared with NPH insulin: • same reduction in HbA1c • less hypoglycaemia overall (but no difference in severe hypoglycaemia) • once daily rather than twice daily • insulin analogues are more effective but more costly • all ICERs outside conventional limits of cost effectiveness • ICERs range from about £100,000 to £400,000 per QALY depending on analogue, gender, complications at baseline and BMI More cost effective to target use of long-acting insulin analogues to people who would be most likely to benefit
Long-acting insulin analogues have few advantages over human NPH insulin in type 2 diabetes, and are expensive • long-acting insulin analogues should be targeted for use in specific individual patients • the widespread use of long-acting insulin analogues for type 2 diabetes may not represent the best use of resources
How are we doing with prescribing? • Effect of NICE guidance ought to be that long-acting insulin analogues are not used routinely, but… • …prescribing data shows extensive uptake • suggests that expensive insulin analogues are increasingly being prescribed instead of human NPH insulin, despite a lack of long-term safety and outcome data
How are we doing with prescribing?http://www.ic.nhs.uk/pubs/prescribingdiabetes0410 COST
Prescribing comparator: Long/intermediate insulin analoguesNHSBSA QIPP Prescribing Comparators http://www.nhsbsa.nhs.uk/PrescriptionServices/3332.aspx • Number of prescription items for long-acting human analogue insulins detemir and glargine as a percentage of the total number of prescription items for all long-acting and intermediate-acting insulins excluding biphasic insulins 98% 38%
Key messages • Management of type 2 diabetes requires individualised multifactorial care • Metformin, a sulfonylurea and human NPH insulin are the preferred hypoglycaemic drugs recommended by NICE • Long-acting insulin analogues have few advantages over human NPH insulin in type 2 diabetes, and are expensive • long-acting insulin analogues should be targeted for use in specific individual patients • the widespread use of long-acting insulin analogues for type 2 diabetes may not represent the best use of resources