Download
1 / 30
300 likes | 502 Views
Glenohumeral Dislocation: Class, Complications and Management. August 21, 2003 Emergency XR Rounds Simon Pulfrey (with much gleaned from Dave Dyck). Normal. Diagnostic Strategies. 1- True AP. 2. Axillary. Transcapular or “Y” View. Post reduction:. Hill-Sachs. Post reduction. Bankhart.

E N D
Glenohumeral Dislocation: Class, Complications and Management August 21, 2003 Emergency XR Rounds Simon Pulfrey (with much gleaned from Dave Dyck)
Diagnostic Strategies • 1- True AP
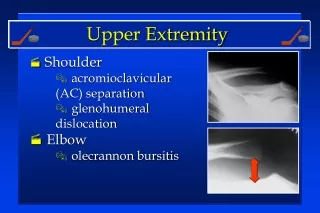
Complications of anterior glenohumeral dislocation and reduction • Neurovascular – neuropraxic and recover in days-weeks • Fractures • Hill-Sachs – 11-50% of ant dislocations. May be higher if consider minor compression fractures • Bankart – ant glenoid rim #. 5% of cases. • Avulsion # of greater tuberosity in 10-15%.
Complications of anterior glenohumeral dislocation and reduction • Rotator cuff injury – 10-15% will have tear. Higher incidence in those >40yrs. • Capsulolabral avulsions in those of younger years
Luxatio Erecta • 0.5% • Usually axial load on abducted arm or indirect trauma • Presents with 100-160 deg of abduction • Humeral shafts lies parallel to spine of scapula (infglenoid lies against chest wall) • Usually need ortho help • Wary buttonhole problem
Posterior Dislocation: -trough sign. Reverse Hill-Sach# on ante-medial hh. -Lightbulb/drum stick
Posterior Dislocation • Rare. 2%. • Commonly missed (50%!) • Seizures, fall on flexed and adducted arm, direct blow • Deceptively normal-appearing AP XR • Increased importance of clinical exam
Clinical Findings: • Arm adducted and internally rotated • The anterior shoulder is flat and the posterior aspect full • Prominent coracoid • The patient won’t allow abduction or external rotation
Rim sign: ant glenoid rim and articular surface of hh increased (usu>6mm)
Summary • Reduce ASAP • Wary neurovascular status, fractures & rotator cuff injuries • Consider necessity of pre & post reduction films on an individual basis • Know well three methods of reduction • Suspect posterior dislocations in appropriate pts