Download
1 / 68
680 likes | 777 Views
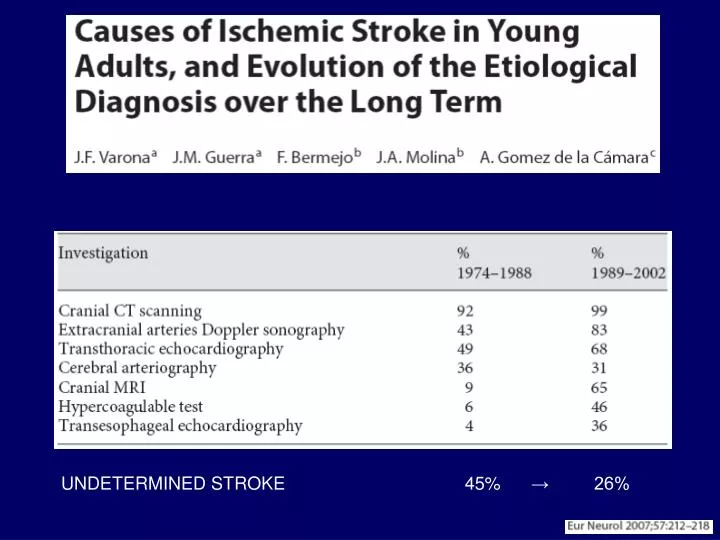
UNDETERMINED STROKE 45% → 26%. STROKE Risk Factors. AGE HYPERTENSION CARDIAC DISEASE → ATRIAL FIBRILLATION → HEART FAILURE DIABETES HYPERCHOLESTEROLEMIA ……. CARDIAC EMBOLISM:.

E N D
UNDETERMINED STROKE 45% → 26%
STROKE Risk Factors AGE HYPERTENSION CARDIAC DISEASE → ATRIAL FIBRILLATION → HEART FAILURE DIABETES HYPERCHOLESTEROLEMIA ……
CARDIAC EMBOLISM: SPECIFIC DISEASES OR CLINICAL SYNDROMES ??
CARDIAC EMBOLISM: The Paradigm of Virchow’s Triad
VESSEL WALL ABNORMALITY BLOOD STASIS HEMOREOLOGIC ABNORMALITIES
CAN Ultrasonography Detect …… ? Vessel Wall Abnormality RHEUMATIC VALVE & HEART DISEASE LV ANEURISM DILATED CARDIOMYOPATHY CONGENITAL HEART DEFECTS ARVD CARDIAC MASS LV HYPERTRABECULATION INFILTRATIVE HEART DISEASE YES
CAN Ultrasonography Detect …… ? Blood Stasis GLOBAL OR SEGMENTAL SYSTOLIC DYSFUNCTION GLOBAL OR LOCAL LOW INTRACARDIAC FLOW LOW OUTPUT STATE - ATRIAL FIBRILLATION - HEART FAILURE - MITRAL VALVE STENOSIS YES
CAN Ultrasonography Detect …… ? HEMOREOLOGIC ABNORMALITIES INCREASED PLATELET ACTIVATION & ADHESION ENDOTHELIAL CELLS DYSFUNCTION INCREASED THROMBIN ACTIVITY - THROMBUS FORMATION
Vessel Wall Abnormality RHEUMATIC VALVE & HEART DISEASE LV ANEURISM DILATED CARDIOMYOPATHY
LV ANEURISM STASIS WALL ABNORMALITY
Vessel Wall Abnormality CARDIAC MASS
VESSEL WALL ABNORMALITY BLOOD STASIS HEMOREOLOGIC ABNORMALITIES CARDIAC MASS: ATRIAL MIXOMA
WALL ABNORMALITY BLOOD STASIS
Vessel Wall Abnormality ARVD LV HYPERTRABECULATION INFILTRATIVE HEART DISEASE
WALL ABNORMALITY BLOOD STASIS
Cardiac Amyloidosis NORMAL AMYLOIDOSIS 26% HAVE CLOTS AT AUTOPSY >70% HAVE RESTRICTIVE CARDIOMYOPATHY/HEART FAILURE 35% HAVE ATRIAL FIBRILLATION
Mean FU : 2 years Conclusions—These results suggest that neither massive RLSh nor massive RLSh with concurrent atrial septal aneurysm is an independent risk factor for recurrent stroke, in either the general or younger stroke populations. (Stroke. 2008;39: 3131-3136.) Stroke. 2008;39:3131-3136
Stroke Stroke + TIA
Blood Stasis GLOBAL OR SEGMENTAL SYSTOLIC DYSFUNCTION GLOBAL OR LOCAL LOW INTRACARDIAC FLOW LOW OUTPUT STATE - ATRIAL FIBRILLATION - HEART FAILURE - MITRAL VALVE STENOSIS
AF PREVALENCE IN STROKE PATIENTS 15 - 20 %
ANNUAL STROKE RATE IN AF: 30 YEARS follow up in the FRAMINGHAM STUDY Overall ischemic strokes 4.5% Disabling Stroke 2.5% Stroke + TIA 7% Stroke + TIA + silent strokes > 7%
THROMBOEMBOLIC EVENTS IN “LONE” AF Author Year Pts. Follow-up (years) Embolic events/%pts/year Paroxysmal AF Kopecky 1997 68 13.4 0.66 Davidson 1989 30 4.9 0.64 Scardi 1997 96 10 0.36 Permanent AF Brand 1985 30 10.9 2.4 Kopecky 1987 21 12.3 0.51 Scardi 1997 49 10 1.3
Stroke rates in control patients of RCT Arch Intern Med 1994;154:1449–57
Stroke rate Major Hemorrage (Hylek)
Primary prevention trials Mean Age 69 years
F1.2, BTG, Fibrinogen, V Leiden not independent stroke predictors in AF
HF as a PRO-COAGULANT state • Fibrinogen, D-dimer, F1.2, AT III • Angiotensin, Endothelin, vWF • NO, Monocythe and Platelet Adhesion vWF, soluble Thrombomodulin, E-selectin, BNP
Emboli in HF are not necessarily cardiac emboli: Hypertension Diabetes Aortic ateroma In situ thrombosis Low output state AF is associated in 25% of HF patients
Stroke and Thromboembolism in HF Trials LVEF < 20% PREVIOUS STROKE INTRACARDIAC THROMBUS
Randomised Trials in HF WATCH STROKE RATE 0.7% Warfarin 2.1% Aspirin HEMORRAGIC EVENTS 5.5% Warfarin 3.6% Aspirin HOSPITALIZATIONS 16% Warfarin 22% Aspirin
ASPIRIN effect in HF TRIAL SURVIVAL THROMBOEMBOLISM Ve-HFT no effect decreased Ve-HFT II no effect no effect SOLVD decreased SD decreased (females) SAVE no effect decreased by 55% WASH no effect, worsened HF no effect WATCH no effect, worsened HF no effect
HF: warfarin risk reduction 50% and ICH = 0.3% HOW TO PROVE OAT BENEFIT IN HEART FAILURE ??
The WARCEF study: a milestone for stroke preventative strategy in HF • 3200 HF pts in SR, LVEF < 35% • Randomised, double blind • Warfarin (INR 2.5-3) vs Aspirin 325 mg • Combined primary endpoint: Ischemic Stroke, • ICH, Death