Download
1 / 23
230 likes | 424 Views
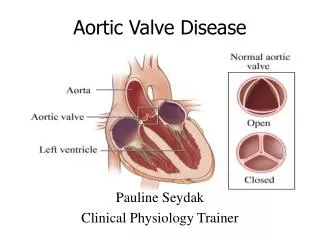
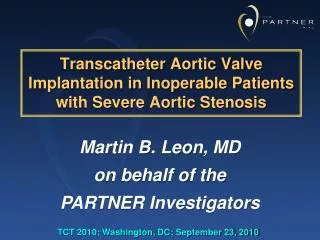
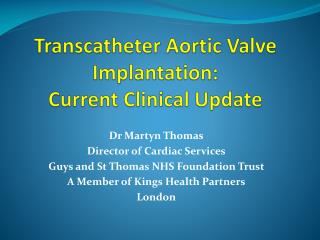
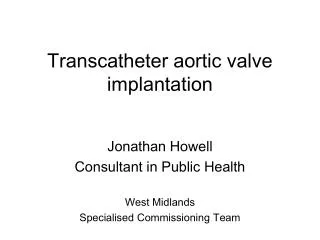
BCIS Autumn Meeting, Crewe, September 2008 Transcatheter Aortic Valve Intervention: How do we take it forward in the UK?. Mark de Belder President, British Cardiovascular Intervention Society. TAVI is simply the latest “new technology” in a long line of new technologies.

E N D
BCIS Autumn Meeting, Crewe, September 2008Transcatheter Aortic Valve Intervention:How do we take it forward in the UK? Mark de Belder President, British Cardiovascular Intervention Society
TAVIis simply the latest “new technology” in a long line of new technologies The real question is: How do we introduce new technologies and take them forward in the UK? …with specific comments related to TAVI
Introduction of new technologies • Clinicians • Identify the problem to be solved • Scientists • Identify the pathophysiological mechanisms at play and potential means of solving the problem • Industry • Seeks investment to develop and implement solutions • Government • Regulates quality of product, safety issues and assesses clinical and cost-effectiveness • National Societies • Encourage and possibly organise appropriate training in procedures • Develop a view on how the treatment should be delivered on a national scale (“Guidelines”) • Assist regulation by collecting audit data with appropriate feedback loops
Pre-clinical: Animal studies Phase I: Initial human experience - Isolated groups working closely with industrial partners; may need to work on redesigns Phase II: Experience in selected units - Can the technique be taught to a larger group? - Initial registries and randomised trials Phase III: Wider take-up - Larger trials demonstrating worth - Followed by widespread uptake Phase IV: Fine-tuning - Are there subsets of patients not previously considered for treatment who could be? Testing of new technologies Trials should not be done too early (during the learning curve) but they should be done
Principles of cost-effectiveness What are you comparing with what? Vs Surgery? Vs Conservative medical therapy?
New technologies: Some make it, some don’t! • Directional atherectomy • Brachytherapy • PICVA? • LAA occlusion devices? • PFO occlusion for migraine?
TAVI: Potential candidates • Patients in whom surgery is deemed too risky (Euroscore >20? >10?) • Risk of surgery outweighs benefits or is not accepted • Prognosis on continuing “conservative treatment” is poor • What is the actual risk in these patients of a percutaneous treatment? • Will the treatment prove efficacious (benefits outweigh risks)? • Patients in whom the risk of surgery is in the “uncomfortable range” (Euroscore 5-10) • Patients at low risk with surgical AVR (Euroscore <5) Treating the highest risk patients first runs the risk of misinterpreting the potential of the technology
TAVI: How should we assess it? • Registries or randomised trials? Or both? • Need to understand the learning curve • Wrong (unethical) to perform a randomised trial of the learning curve of a new treatment with an established older treatment • Early registries bring about refinements in technique and technology In essence, definitive (Phase 3 and 4) randomised trials should not be done without the equivalent of Phase 1 and 2 studies.
TAVI: How should we assess it? • Registry with 1st year mortality of 40% should not put us off if the expected mortality of the cohort was 60% or more • It would put you off if the 1st year mortality was 40% when the expected mortality of the cohort was 20% • It would put patients off if longer term gains are only accrued at an unacceptable early hazard Early studies allow us to inform patients correctly and help us design randomised trials at the right time
TAVI: How big will it get? • What is the current need? • Do we have a clear view of the epidemiology of AS? • Can we evaluate short-, medium- and long-term need with regard to issues of incidence and prevalence? • Do we need to develop a treatment that is better tolerated than current surgical techniques, has fewer complications, and that provides good long-term results? • Even if not “better” than conventional surgery, is it an acceptable option (because of lower procedural risks?) • Or is this a case where the clinical “need” is being pushed by industry? • Industry estimate for the UK is ~2000/annum = ~30-35pmp • But clearly more if it is extended to lower risk groups • What will patients want? • Discussions with sick or elderly patients with AS (3 groups)
Mitral Balloon Valvuloplasty BCIS data: 2000-2006
2006 data: Ludman Mitral Balloon Valvuloplasty 2006: 139 procedures/28 centres
TAVI: Starting up • What are our motives for starting a TAVI programme? • Because we want to get it going before centre Y does it • Because it will bring income in to my Trust (will it?) • Because I’m bored just doing coronaries • Because we genuinely believe that this is a technology that will last and will provide an option to patients that is not currently available?
TAVI: Starting up • Have we got the infrastructure to set it up? • Lab space (hybrid lab?) • Committed multidisciplinary team • Approved business case • Training • Wet labs • Proctoring (international and UK-based) • Patients • How do we identify patients that want to be in the first wave within the unit? How do we get their consent? • Does proctoring minimise learning curve issues?
TAVI: Randomised trials • Do we really need a randomised trial of TAVI vs medical treatment for those deemed at too high a risk for surgery? • Will surgeons engage with a trial of TAVI vs AVR in patients they are currently not keen to treat? • Pilot studies in a small number of units will be needed before setting up a randomised trial against surgery in those currently operated on.
TAVI: “Purity” vs “Pragmatism” • Did cardiac surgeons perform randomised trials on: • AVR? • MVR? • Aortic root replacement? • VSD closure? • Pulmonary endarterectomy? • etc
TAVI: Commissioning issues • Tariff • Meeting with DoH/Industry/PbR team • Commissioning • Meeting 17th September 2008 (East Midlands Specialised Commissioning Group) • only within the confines of an RCT is inappropriate • Specialist commissioning • Population base • Minimum population 1 million? • Keep under review
TAVI: NICE • Meeting (early 2008) between IPAC and: • BCIS • SCTS • HRUK • BCCA • NICE IPG • Importance of data collection: • Industry-sponsored registries • UK dataset via CCAD • Import data collected to date
Transcatheter Valves 2007 data: Ludman • TAVI Dataset agreed • Collection via CCAD • Web browser interface • Version: 3.5 • Available from BCIS web site (www.bcis.org.uk)
Agencies with potential interest • MHRA • Quality Control • NICE • Clinical and Cost-Effectiveness • Interventional Procedures Advisory Committee • Part of NICE • Has replaced SERNIP (Safety and Efficacy Registry for New Interventional Procedures) • Academy of Royal Colleges • National Specialist Commissioning Advisory Group (NSCAG) • Regional Specialist Commissioning Groups • NHS R&D Directorate • Health Technology Assessment Programme (HTAP) • Standing Group for Health Technology Assessment (advisory group) • Health Commission • Central Cardiac Audit Database
UK Centres - 2006 PCI (91) Who? Where? How many? Inter-hospital referral
Personal view • TAVI should not (at this stage) be done by all centres • TAVI should not be done by all operators • Need to identify agreed standards (UK, International): • Characteristics of the Institution • Characteristics of the operating teams and support infrastructure • Volume of activity and results
BCIS Council BCIS Data Monitoring Committee • New dataset for TAVI now available • Datasets for other non-coronary interventions are needed • Persuade operators to conform to process • Work with agencies to ensure a quality service for UK patients