Download

1 / 47
470 likes | 542 Views
Learn iron absorption, types of hemochromatosis, diagnostic methods, symptoms, and treatment options for this genetic disorder affecting iron metabolism and leading to organ damage. Early detection is crucial.

E N D
Hemochromatosis Dr.moosavi Abadan-Khordad-1397
OBJECTIVES • Review iron absorption and transport • Describe types of hemochromatosis • Hemochromatosis and the laboratory • Suspicion • Investigation • Diagnosis
Background • Iron is an important nutrient, but too much can be bad • Absorb about 10% from our diet • Individual with this disease absorbs about 30% • No mechanism to eliminate iron • Excess damages liver, heart, and pancreas
Fe+3 Fe+2 Fe+3 Fe+2 Fe Fe Transferrin Fe Fe Villus enterocyte Fe2+ Fe+2 Fe+3 Ferritin Macrophage Ceruloplasmin Bone Marrow Liver
3 - 4 g 1 – 2 mg 1- 2 mg Total body iron Daily iron absorption Daily iron loss OTHER Menstrual (monthly) pregnancy (total) Normal Iron metabolism Male Female • 2 - 3 g • 1 – 2 mg • 1- 2 mg OTHER • 20 - 40 mg • 600 - 900 mg
Fe+3 Fe+2 Ferritin 1 – 2 mg /d 1 – 2 mg /d Macrophage Fe Fe Fe2+ Villus enterocyte 20 mg / d Liver Menstruation 20 – 40 mg /m Bone Marrow
Fe+3 Fe+2 Ferritin 7 – 8 mg /d 1 – 2 mg /d Macrophage Fe Fe Fe2+ Villus enterocyte 20 mg / d Liver Menstruation 20 – 40 mg /m Bone Marrow
Iron transport and absorption proteins • Transferrin • Ferritin • Transferrinreceptor • Ceruloplasmin
Non-heme iron absorption process • Reduction of ferric to ferrous iron • Transport across brush border • Sequestration in enterocyte • Basal transport from cell • Oxidation to ferric form • Transport by transferrin • Uptake by transferrin receptors • Utilisation or storage
Different Forms • Primary or hereditary • Secondary • Juvenile • Neonatal
Classical Hemochromatosis • First description 1865 • inherited disorder 1935 • autosomal recessive disorder of excess iron deposits in parenchymal tissues causing organ damage and dysfunction • Affects liver, pancreas, heart, joints, pituitary, skin – “bronze diabetes” • Considered rare disease of elderly men
Hemochromatosis by 1996 • Syndrome preventable if iron overload diagnosed and treated early. • Treatment simple: - phlebotomy • Recognition – high transferrin saturation and ferritin • Studies of blood donors suggested that 1:200 to 1:400 people have biochemical iron overload • Much more common than originally thought • 1 in 200 in NW European populations
Hereditary • HFE is gene for protein that regulates iron absorption • 2 mutations: C282Y and H63D
HFE B C E A HLA genes C282Y mutation in HFE gene In late 1996 an HLA linked gene on chromosome 6 p 21.3 was found to be associated with hemochromatosis patients of North West European origin
Early Stage Symptoms • Arthritis • Fatigue • Abdominal pain • High blood sugar • Hypothyroidism • Weight loss
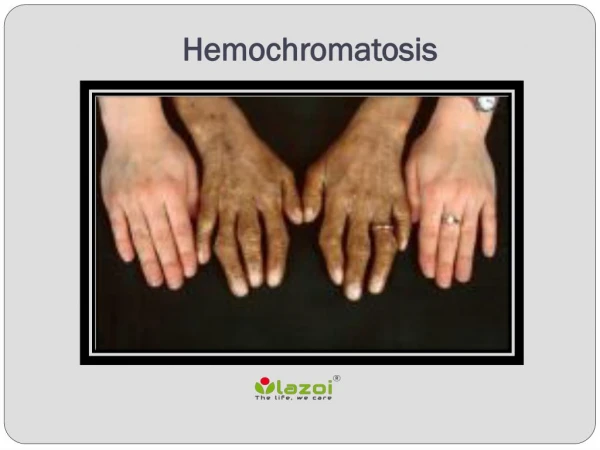
Advanced Stage Symptoms • Liver disease • Liver cancer • Diabetes • Cardiac arrhythmia • Congestive heart failure • Discolored skin
Clinical Manifestations • Influenced by • Age • Sex • Dietary iron • Alcohol • Blood loss in menstruation and pregnancy • Unknown factors • Alcohol abuse and Hepatitis C accelerate • Classic description: cutaneous hyperpigmentation and diabetes in a patient with cirrhosis
Classic Triad: • Cirrhosis (hepatic damage) • Diabetes (type II) (pancreatic damage) • Bronzing of skin (hyperpigmentation) • Traditional triad means diagnosed too late! • Damage may be only partially reversible • Goal is to detect the disease BEFORE organ damage occurs
Hepatocellular carcinoma • During follow-up, hepatocellular carcinoma developed in 28 of the 97 (28.8%) patients with cirrhosis but in none of those without • The risk was increased significantly in patients > 55 yrs, those with HBS Ag and alcohol abuse Prognostic factors for hepatocellular carcinoma in genetic hemochromatosis. Hepatology 1994 Dec;20(6):1426-31
Diagnostic testing for HH • Transferrin saturation: • >45% indicates significant Fe accumulation • Serum ferritin -levels indicating significant iron accumulation: • >150 mcg/L pre-menopausal women • >200 mcg/L post-menopausal women • >200 mcg/L for men • Liver biopsy if ferritin >1000 to assess damage Consider genetic testing – DNA testing for common mutations (C282Y, H63D)
Iron overload in liver Pearls’ Prussian blue stain of a liver biopsy from a patient with hereditary hemochromatosis. Left panel: low-power viewshows intense iron stainingof hepatocytes. The blue-stained iron depositstypically start at the periphery of the liver lobule and extends centrally. Right panel: high-power view shows intense on staining (in blue) of hepatocytes. Courtesy of Stanley L. Schrier, M.D.
Hepatic Iron Index (HII) in hemochromatosis - the hepatic Iron index in four groupsof patients: normal controls, alcoholic liver disease, pre-fibrotichemochromatosis, and fibrosis and cirrhosis caused by hemochromatosis. Among the patients with hemochromatosis, the opens circles represent heterozygotes, andthe close circles represent homozygotes. The HII iscalculated by dividing the hepatic iron concentration bythe patients age in years. Allpatients with homozygoushereditary hemochromatosis had an hepatic I index > 2, alevel not seen in the otherpatients. Hepatology 1986; 6:24
MRI Liver • Slow (approx 20 mins) • Relatively simple • Good correlation with iron levels and cirrhosis
Genetic Testing for HHShould be offered to those patients with: • Appropriate clinical presentation • Elevated transferrin saturation and ferritin • Liver biopsy suggestive of iron overload • First degree relative of a known case *Must be offered to an affected family member or index case FIRST
What is the value of genetic testing? • To confirm diagnosis • Sequential screening of family members
“So if I have the gene…I’ll get the disease” • Not necessarily! • This statement refers to an important concept in genetics • Penetrance • The proportion of individuals with a mutation causing a particular disorder who exhibit clinical symptoms of that disorder
Mutated HFE Genes = Hemochromatosis? No, because of • Incomplete penetrance: • Even though some individuals have the susceptible genotype they may never manifest symptoms of the disease due to: • Environmental factors: blood donation • Genetic factors: other modifying genes • Low penetrance for C282Y homozygotes
Indications to consider hemochromatosis • Apply to classical Type 1 Hemochromatosis • General guidelines – indications for genetic testing • Based on fasting transferrin saturation as the primary biochemical screen Guidelines: Iron Overload 2001
When to consider the diagnosis? Adult onset diabetes Arthritis Unexplained cirrhosis or persistently raised liver enzymes Congestive heart failure or cardiomyopathy Secondary hypogonadism Increased skin pigmentation Not in guideline Severe fatigue Arthralgias
Genetic Testing and Treatment • First degree relatives of confirmed hemochromatosis patients can have the genetic test done directly • If iron overloaded and not C282Y homozygous consider other causes • Management (phlebotomy) is dependent on the ferritin level not the transferrin saturation • Phlebotomy - till ferritin around 50 µg/L
No Fasting morning TS >50% Stop Yes No Repeat TS and serum ferritin > normal Check in 12 mo Yes Yes Secondary Iron Overload? Rx & Recheck No HFE gene testing; C282Y homozygote? Yes 1. Normal AST2. Ferritin <1000 ug/L3. No hepatomegaly No No Yes Phlebotomy Liver Biopsy - positive for HHC Yes No Phlebotomy Follow
Medical Management • The goal - detect patients before symptoms of iron overload. • Phlebotomy weekly or biweekly • Check ferritin every ~10 phlebotomies • Stop frequent phlebotomy when ferritin 25-50mcg/L • Maintenance phlebotomy every 3-4 months • Dietary recommendations • Consider hematology or GI consult for confirmed cases to guide treatment and monitoring
Chelation therapy for HHC with deferoxamine can also lead to clinical improvement, however, it is almost never necessary
Diet • Realistically little role • Avoid large quantities Vitamin C • Increased Fe absorption • Increases Fe release from storage sites • Rare reports of inducing lethal cardiac failure