Download
1 / 53
760 likes | 2.38k Views
Peroneal Tendon P athology. Christina Sigur DPM Intermountain Medical center Salt Lake City, UT. Overview. Anatomy, Etiology, MOI Classification Clinical Diagnostic tools Clinical conditions and treatments. Peroneal Tendon Pathology. ANATOMY. Anatomy. Origin

E N D
Peroneal Tendon Pathology Christina Sigur DPM Intermountain Medical center Salt Lake City, UT
Overview Anatomy, Etiology, MOI Classification Clinical Diagnostic tools Clinical conditions and treatments
Peroneal Tendon Pathology ANATOMY
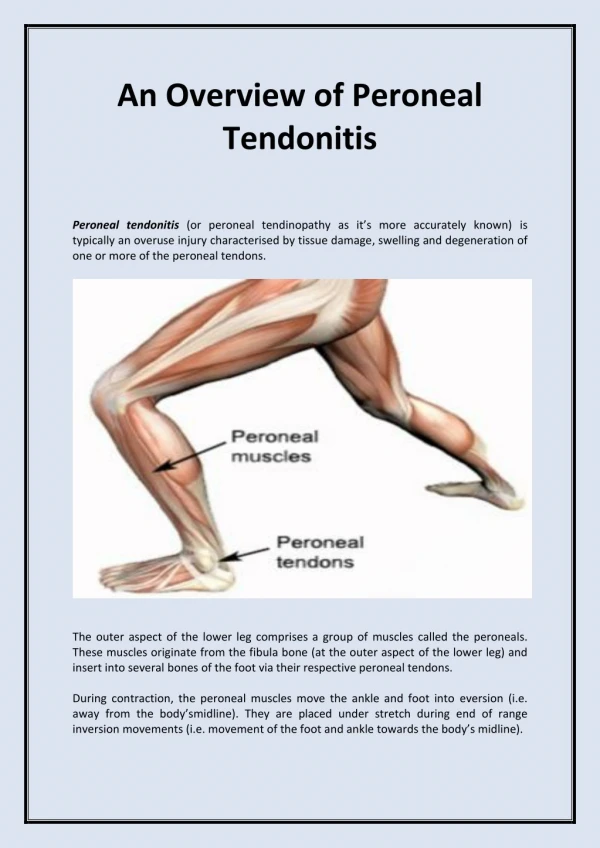
Anatomy • Origin • PL: lateral condyle of the tibia and fibular head • PB: fibula, middle third of the leg • Pathway: • Share a common sheath 4cm proximal to tip of lateral malleolus • Then pass through a retromalleolar groove or fibro-osseous tunnel until reaching the tip of the lateral malleolus • PL lying posterolaterally to PB • Then separate into individual sheaths • PL passes under peroneal tubercle/IPR, enters 2nd tunnel (long plantar ligament and cuboidperoneal groove), insertion 1st MT/medial cuneiform • PB passes over peroneal tubercle/CFL, insertion 5th MT base Cerrato & Myerson, Foot Ankle Clin N Am 14 (2009) 299-312
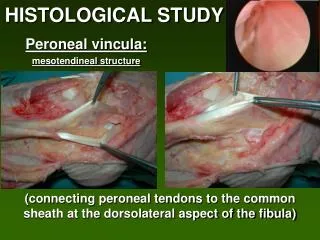
Anatomy • Fibro-osseous tunnel • Anterior wall: fibula • Posterior wall: deep fascia of the leg and calcaneofibular ligaments • Medial wall: posterior talofibular and calcaneofibular ligaments • Lateral wall: SPR Cerrato & Myerson, Foot Ankle Clin N Am 14 (2009) 299-312
Anatomy Superior peronealretinaculum • 1-2cm wide , originating 1cm proximal to posterolateral fibular tip inserting into lateral wall of calcaneus • Primary restraint to tendon subluxation Peroneal tubercle (Hyer et al. 2005) • Function • Fulcrum directing the PL tendon toward the cuboid • Insertion site for the inferior peronealretinaculum • Separates the sheaths of the PB and PL tendons • Hypertrophymechanical stress • Gliding facet on inferior side for PL
Anatomy Fibular malleolar groove - controversial No difference detected in shape between pts with and without pathology (Adachi et al 2009) Flat or convex shape predisposition to subluxation? (Ogawa et al 2007) Muscle belly or accessory muscle low-lying PB muscle belly ( or peroneusquartus muscle (incidence 6-22%)stenosis within groove, attenuation of SPR
Anatomy • Avascular zones • PL: 1. turns around the lateral malleolus, extending to the peroneal tubercle 2. turns around the cuboid • PB: 1. turns around the lateral malleolus • Factoid: Oxygen consumption of tendons and ligaments 7.5 times lower than muscle Selmani et al. FAI Vol 27(3) March 2006
Peroneal Tendon Pathology biomechanics
Biomechanics • 63% hindfooteversion • 4% total plantarflexion • Dynamic stabilizers of the lateral ankle ligament complex • Cavovarus foot type places PL at mechanical disadvantage • Reduction of moment arm • Increasing frictional forces • Brandes and Smith: 82% patients with PL tendinopathy had cavovarushindfoot position Brandes and Smith. FAI. Vol 21(6) June 2000
Peroneal Tendon Pathology Clinical assessment
Clinical Assessment Pain exacerbated by passive RF inversion and passive ankle plantarflexion, active eversion/dorsiflexion Persistent swelling along peroneal tendon sheath Some complain of medial foot pain Snapping sensation Ankle Instability Chronic ankle pain Retromalleolar /posterolateral pain Dombek et al. – 60% peroneal disorders were accurately diagnosed at 1st clinical visit
Clinical Assessment • Palpation to identify tender areas • Test peroneal muscle strength • Evaluate for sural neuritis • Peroneal tunnel compression test • Knee flexed at 90 degrees, foot in a resting plantarflexed position, while manual pressure applied to retrofibular region – pain? • Have pt p/f the 1st ray – loss or limitation? • Elicit dynamic tendon instability • Coleman block test – RF varus?
Peroneal Tendon Pathology:Differential Diagnoses Sinus tarsi syndrome Fracture – fifth metatarsal base, cuboid, fibula Calcaneocuboid syndrome Talar OCD lesion Ankle/subtalar loose bodies DJD Sural neuritis Radiculopathy Accessory muscle/bone Tarsal coalition Heckman et al. J Bone Joint Surg Am 2008; 90:404-418
Peroneal Tendon Pathology imaging
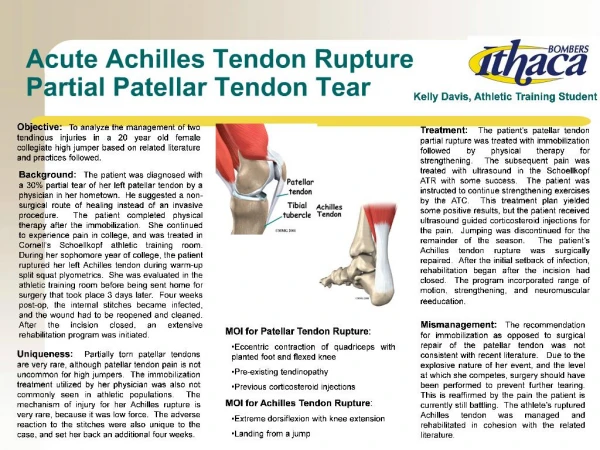
Imaging • Radiographs • AP, lateral, calcaneal axial • Assessment: Hypertrophied tubercle? Fracture (46%)? Os peroneum? Bony spurring? Arthroses? Fleck sign? • MRI – modality of choice • T2 signal - 92% sensitivity, 79% specificity • Findings of tear: heterogeneity/discontinuity of tendon, fluid-filled • Linear or round increase signal in tendon • Caution: Magic angle – artifactual signal in tendon fibers oriented at 55 degrees to magnetic field axis • CT – bony abnormalities Klein et al. FAI Vol 29(10) Oct 2008
Imaging • Ultrasonography • Noninvasive, no radiation, interactive • Inexpensive – 19% of MRI cost • 90-100% accuracy, 85-100% specificity, 100% sensitivity • Description: diffusely enlarged hypoechoic without defects • Normal: uniformly echoic lines on longitudinal images • Can differentiate between tendinosis and tenosynovitis (echogenic foci) • Peronealtenography Grant et al. J Bone Join Surg Am. 2005;87:1788-94
Imaging Ultrasound and Surgical Criteria Normal = OUniformly parallel echogenic fibrils. Normal appearing tendon. Tendinosis = I Diffusely enlarged hypoechoic tendon or hypoechoic foci within the tendon that do not extend to its surface. Enlarged/inflamed tendon. Partial Tear = II Clefts or linear hypoechoic gaps within the tendon substance that extend to the periphery. Partial-thickness visible tear. Complete Tear = III Discontinuity of the tendon or complete nonvisualization of the tendon. Complete visible tear with or without retraction. Grant et al. J Bone Join Surg Am. 2005;87:1788-94
Peroneal Tendon Pathology Tendinitis/tendinosis
Peroneal Tendinitis/Tendinosis • How to differentiate • Tendinosis: palpable mass that moves with the tendon • Tendinitis: fluid around tendon without tear
Peroneal Tendinitis/Tendinosis:Treatment • Conservative • NSAIDs, RICE, lateral heel wedge for primary RF varus, lateral forefoot post for primary FF valgus • Cast immobilization in rigid AFO/SLC/CAM walker for 6 weeks • Surgical • Open tenosynovectomy, examine tendon intraop, debridement of tendon if needed • Smooth hypertrophied peroneal tubercle • Tendon sheath is left unrepaired • Postop: NWB in SLC for 2 weeks (foot p/f and everted), WB at 2 weeks, discontinue castboot at 4-6 weeks, ROM/strengthening at 2-4 weeks Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Peroneal Tendon Pathology Os peroneum syndrome
Os Peroneum Syndrome:Numerous Definitions… Acute fracture of osperoneum or diastasisof multipartite osperoneum Chronic fracture of osperoneum with associated stenosingtenosynovitis of PL Partial or complete rupture of PL tendon near osperoneum Entrapment of PL tendon and osperoneum by a hypertrophied peroneal tubercle Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Os Peroneum Syndrome Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Os Peroneum Syndrome:Treatment • Conservative • Surgical • Os peroneumexcision • Reinforce tendon or repair as needed
Peroneal Tendon Pathology Tendon tears
Peroneal Tendon Tears: Mechanism of Injury PeroneusBrevis tendon PeroneusLongus tendon Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009 • Incompetent SPR • Subluxation of PB as result of laxity/tear of SPR, causing splay or split over sharp posterolateral edge of fibula • Compression of PB tendon between posterior fibula and PL tendon during inversion injury or repetitive loads • Low-lying PB muscle belly or accessory muscle, increased strains over tendons Incompetent SPR Sudden inversion sprain or forced eversion of supinated foot Avulsion fracture of osperoneum with diastasis and proximal retraction of tendon or sesamoid itself Cavovarus/rearfootvarus deformity
Peroneal Tendon Tears: Classification Classification system (Krause and Brodsky) • After debridement of damaged portion of tendon • Grade I : <50% of cross-sectional area and tendon repair is recommended • Grade II: >50% of cross-sectional area and tenodesis is recommended • Tenodesis performed 3-4cm proximally above lateral malleolus tip and at least 5cm distally to avoid fibular impingement
Peroneal Tendon Tears:Treatment algorithm (Redfern and Myerson) • I Both tendons are grossly intact • Excision of the longitudinal tear and tubularization of the remaining tendon • II One tendon is torn and irreparable and the other tendon is functional (has sufficient excursion) • Tenodesis performed proximally between the peroneuslongus and peroneusbrevis • III Both tendons are nonfunctional • No excursion of the proximal muscle Tendon transfer. • Excursion of the proximal muscle and no tissue bed scarring One- stage tendon graft • Excursion of the proximal muscle with tissue bed scarring Staged tendon graft with silicone rod Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Peroneal Tendon Tears:Treatment for chronic tears • Wapner et al 2006 - Staged reconstruction using Hunter rod and FHL transfer • Objectives: • Create viable tendon sheath allowing free movement of the new tendon • Re-establishment of the stability of the retinaculum • Provide dynamic replacement for the peroneal tendons
Peroneal Tendon Tears:Other considerations • Correct associated pathology • Chronic ankle instability • Osteophytes • Hindfootvarus
Acute Peroneal Tendon Ruptures:Treatment End-to-end suture Transfer of FDL to the PB tendon Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Peroneal Tendon Pathology Dislocation/subluxation
Peroneal Tendon Dislocation/Subluxation:Mechanism of action • Inversion injury of the dorsiflexed ankle with concomitant contraction of the peroneals SPR injury • Disruption of ankle ligaments causing more stress on SPR • SPR is secondary restraint to ankle inversion • Anatomical variants 1 • Extension of PB muscle into fibular groove • Shallow retromalleolar groove • Variable SPR • Congenital deformities, bony
Peroneal Tendon Dislocation/Subluxation:Classification • Eckert and Davis (3 Grades of anatomic injury) • I: SPR with the periosteum stripped off the lateral malleolus (51%), PL dislocated anteriorly • II: SPR elevated + elevation of distal 1-2cm of dense fibrous ridge of the lateral malleolus (33%) • III: SPR elevated + elevation of thin fragment of bone anteriorly along the fibrous ridge from fibula (16%) • Oden modification • IV: SPR elevated from the posterior insertion at calcaneus
Peroneal Tendon Dislocation/Subluxation:Acute Injury Treatment • Conservative • Cast immobilization • In slight inversion • Indicated for gradeI and possibly gradeIII • Heel lifts, taping, orthoses, PT rehab • Surgical • Percutaneous stabilization • Summers et al 2008
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment • Conservative – not advised • Surgical • Anatomic re-attachment of the SPR • Soft tissue reconstruction to reinforce SPR • Re-routing of tendons under CFL • Bony procedures • Groove-deepening • Bone-block
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment Soft tissue repair • Direct repair of the SPR • Superior retinaculoplasty (Adachi et al 2006) • Use of local or transplanted tissues to reconstruct the retinaculum • Watson-Jones: Elevate osteoperiosteal flap posteriorly from the lateral fibula to deepen sulcus and create a pedicle of the SPR and fascia of the FHL • Jones: Using an Achilles tendon strip anchored through drill hole in lateral malleolus Heckman et al. The American Journal of Sports Medicine, Vol 37 No 3 2009
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment Re-routing procedures • Substituting the CFL for the retinaculum • Poll and Duijfjes – transposition of CFL from its calcaneal insertion, re-route peroneals under the ligament, then replace • Disadvantages 61% complication: ankle stiffness, decreased ankle inversion • Wang et al (2009)- 2mm drill bone hole, elevate CFL with bone block, transposed with another bone block, moved in more anteriorly, peroneal tendons looped under the CFL • Postop NWB 4-6 wks, early rehab, early return to work/sports
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment Bony procedures • Bone-block procedures • Use of bone graft as physical restraint – sagittalosteotomy within fibula, posterior displacement • Disadvantages: tendon adhesion to fresh bone wound/irritation, fractures of bone graft, need for hardware • Michelli et al 1989 – 11/12 good results
Peroneal Tendon Dislocation/Subluxation:Chronic Injury Treatment • Fibular groove deepening • Raising osseous flap posterolateral fibula, removed underlying cancellous bone, reducing flap, impacted with bone tamp, relocate rendons, repair SPR • Ogawa et al 2007 – indirect method, less traumatic – intramedullary reaming then impact thinned fibular cortex • Preservation of periosteum • Walther et al 2009 – retromalleolar groove impaction
Peroneal Tendon Dislocation/Subluxation:IntrasheathSubluxation Thomas, et al JFAS Vol 48(3) May/June 2009 • Subluxation within tendon sheath • High incidence of low-lying muscle belly • Treatment • Repair tendon pathology • Resect low-lying muscle belly or accessory tendon 2-3cm proximal to fibro-osseous tunnel using electrosurgery • Deepen peroneal groove • SPR repaired
Peroneal Tendon Pathology: Conclusions Remember anatomy Take a good history and physical and be highly suspicious Multiple pathologies at once