Download
1 / 61
650 likes | 1.42k Views
AEP Monitor 麻醉知覺/深度監測儀 ( Auditory Evoked Potential). 台大醫學系六年級 全以祖. Contents. 1、前言 2、 AEP Monitor 的理論及臨床應用 3、 AEP v.s. BIS 4 、WHY AEP?. 有人說:. 麻醉醫師的工作流程非常類似〝 Pilot 〞 不同的是 -- pilot 已有非常精確及〝直接〞且〝即時〞的自 動導航系統、全球衛星定位系統… etc. 。 -- pilot 有非常嚴格的工作時間限制。

E N D
AEP Monitor 麻醉知覺/深度監測儀 (Auditory Evoked Potential) 台大醫學系六年級 全以祖
Contents 1、前言 2、AEP Monitor的理論及臨床應用 3、AEP v.s. BIS 4、WHY AEP?
有人說: 麻醉醫師的工作流程非常類似〝Pilot〞 不同的是-- pilot 已有非常精確及〝直接〞且〝即時〞的自 動導航系統、全球衛星定位系統…etc.。 -- pilot有非常嚴格的工作時間限制。 然 而 -- 麻醉醫師只有一些輔助儀器〝間接〞且〝非即 時〞來提供病患麻醉深度/知覺的判斷。 -- 麻醉醫師常overtime。
有人說: 麻醉是一種 Science 更是一種 Art 如何在安全、品質、成本間取得 最佳的 Result,仍是最主要的目標?
各位麻醉醫師在過去的經驗中,是否仍有一些有待挑戰的Subject呢?例如:各位麻醉醫師在過去的經驗中,是否仍有一些有待挑戰的Subject呢?例如: 1、在Induction時,提供的劑量是否夠或不夠?可否 intubation了 或再等一下? 2、多種藥物的交互作用下,對麻醉深度的影響到底為何? 3、在maintenance期,血壓亦或心跳升高,是否深度不夠,亦 或其他原因呢? 4、在reversing期,如何判斷病患意識已開始恢復,可被喚醒了? 5、在maintenance期,何時可減量麻醉氣體,以提早reverse patient?
各位麻醉醫師在過去的經驗中,是否仍有一些有待挑戰的Subject呢?例如:各位麻醉醫師在過去的經驗中,是否仍有一些有待挑戰的Subject呢?例如: 6、如何在OB或 Truma Cases中,更能掌握病患麻醉深度呢? 7、如何在低溫Open-Heart中,更能掌握病患麻醉深度呢? 8、做Low-Flow時,能否告知麻醉深度,以便更能掌握呢? 9、目前麻醉環境中,是否就是缺少一個〝直接且即時〞告知麻 醉深度的設備呢?
The patient • The patient has 2 worries: • 1: Will he sleep during the operation? • 2. Will he wake up after the operation?
Basic basic basic basic basic • The hearing is the last sense that leaves and the first that returns during anaesthesia. • AEP is just the brain response to a click stimuli through the hearing nerve • AEP is a very weak electrical signal wrapped in the EEG background actvity. • Let’s look at how tiny tiny this signal is.
Why monitor sleep?It is important to think about this. • The implications of undersedation • Patient remains immobilized but feels pain • Although it is occurs in only 0.1% - 0.2% of all surgeries, 23 million surgeries are performed in the U.S. each year • Resulting in 35,000 cases of surgical awareness • The implications of oversedation • To avoid the possibility of surgical awareness too much hypnotics and analgesics may be administered • The patient’s recovery time is extended: higher room cost • More drugs than necessary are used: higher drug cost
Burst Suppression We look at spikes < 3,5 uV. In contrast: An awake Pa amplitude is typically 0.7 uV. And, an asleep amplitude is typically 0.4 uV
400 x 40 x ECG signal has approx. 400 x amplitude than the AEP signals. EEG signal has approx. 40 x amplitude than the AEP signal
Extracting the evoked responseBefore A-Line it took too long to ”detect and present” (extract) this weak signal, because it requires advanced signal processing 1 click 128 clicks 256 clicks 1024 clicks click 100 ms
But, lets make this more visible Let’s see what happens when we send a click through the ear.
Position of electrodes A deviation in the positioning of the electrodes up to 2 cm does not have significant influence on the ARX-index.
Place Headphones To Monitor Some prefer to wait with the headphones until electrodes are connected
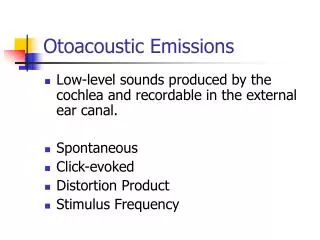
FIGURE 35–10 Schematic of auditory neural pathway. The BAEP is initiated by stimulation of the cochlea with a broadband click stimulus given via an ear insert in the external auditory canal. Neural generators of the BAEP peaks are shown.
Frontal cortex and association areas Medial geniculate and primary auditory cortex Acoustic nerve and brainstem
What does the AEP Look Like? Pa Pa latency + 0.1µV Pa amplitude Nb 100 msec
Frontal cortex and association areas Medial geniculate and primary auditory cortex Acoustic nerve and brainstem
American Encephalography Society Criteria for Retrochochlear Dysfunction • 1. Abscencr of all waves • 2. Absence of all waves following wave I or II • 3. Increase of I-V interpeak interval • 4. Decrease of V/I amplitude ratio • 5. Interaural I-V interval asymmetry
Pa Nb And, of the opposite during awakening
P P P P P P P P 1 1 1 1 Pa Pa Pa Pa Po Po Po Po No No No No Na Na Na Na Nb Nb Nb Nb 7 7 N N N N 1 1 1 1
Patient-Related Factors • 1. Age • 2. Temperature • 3. Drug Effects - Barbiturates, Benzodiazepines - Fentanyl - Ketamine, N2O - Isoflurane - Halothane, Enflurane
Desflurane Pa 1.5% Nb 3% 6% The AEP during Anaesthesia With kind permission from Dr Christine Thornton, Northwick Park, London, UK.
Effect of intubation on the AEP Pa + 0.1µV Nb Post-intubation Pre-intubation 100ms With kind permission from Dr Christine Thornton, Northwick Park, London, UK.
The Effect of Midazolam on the AEP Awake Nb Loss of eyelash response 0 50 100 Time (ms) With kind permission from Dr Christine Thornton, Northwick Park, London, UK.
The effect of propofol on the AEP Response to command Nb No response to command 0 50 100 Time (ms) With kind permission from Dr Christine Thornton, Northwick Park, London, UK.
Conclusions • Graded changes with depth of anaesthesia • Similar changes for different anaesthetics • Shows response to noxious stimulation • AEP indicates level of consciousness • Technology has been studied since early 1980’s
1 2 3 4 5 6 7 8 . . . . . . . . . . . 239 . . . 256 257 Moving time Averaging and ARX ARX -model MTA 256 sweeps MTA 18 sweeps
mv 0,1 mv 0,2 mv 0,3 mv 0,4 Total 3,7 x factor = 100 Index calculation? AEP window = 20-80 ms xixi+1
Index calculation • So, then you have a real curve, the index is high = 93 • And, an almost flat curve gives a low index = 16
What it is • AAI is typically higher than 60 when the patient is awake and decreases when the patient is anaesthetised; loss of consciousness typically occurs when the AAI is below 30
What we did • The click detection is achieved by estimating the Signal to Noise Ratio (SNR). • The SNR is defined as the ratio between the measured signal and the noise. • The SNR threshold is 1.45; this means that when the SNR is above 1.45, the quality of the AEP is satisfactory. • On the other hand if the SNR is below 1.45, the signal quality is low, and a further averaging of the AEP is carried out. • Yet if this does not improve the SNR, the symbol LOW AEP or NO AEP will appear on the monitor.
What we did • The symbol NO AEP and flashing AAI will appear in one of the following situations: • The Headphones are disconnected or not working properly. • The subject may be hearing impaired. • Too much noise is present. Check grounding of the AAI monitor and the surrounding equipment. • The subject has very high levels of EMG activity, meaning that the AEP is embedded in an excessive amount of noise, impeding the extraction of the AEP.
What we did • The symbol LOW AEP will appear frequently during anaesthesia in one of the following situations: • both the AAI and the SNR are low. • a considerable suppression of the AEP is taking place caused by the effect of the anaesthetics.
What we did • Caution should be taken if LOW AEP appears in an awake subject as this indicates one of following situations and renders the AAI unreliable: • The Headphones are disconnected or not working properly. • The subject may be hearing impaired. • Too much noise is present. Check grounding of the AAI monitor and the surrounding equipment. • The subject has very high levels of EMG activity, meaning that the AEP is embedded in an excessive amount of noise, impeding the extraction of the AEP.
What we did • For both LOW AEP and NO AEP: The response time after the headphones are disconnected until LOW AEP or NO AEP appears in the display has a mean value of 50 seconds and 97 % of the response times will typically be below 2 minutes.
A good case • Just to illustrate how important it is. • Customer couldn’t understand why the index was high? • Complained that “something was wrong” • All details captured by our man • After downloading and descriptions the clinicians agreed the anaesthesia was not optimal. • They could actually see things they never seen before
Fentanyl 0,15 + Pentothal 250mg Intubation. + Sevo FI 0,2 Start surgery. Gyn. Lap. procedure . FI 1,0 + MAC 1,0 Moved Patient on table Tracrium 15mg Index dropped and NMB was given to prepare intubation TIVA with induction and Maintenance would have prevented this Patient still not deep enough and reacts. Remember: 50% sleep at 1 MAC Intubation too soon. Fentanyl had not reached peak effect. Induction started with normal doses Penthotal dose was small for this patient. Gas conc. too low Patient was not deep enough to be moved on table. Dose of gas too low.