Download
1 / 56
720 likes | 1.48k Views
LIVER - Normal histology - Cirrhosis. 8 th November 2007 Dr. Cynthia Heffron Clinical Lecturer in Histopathology. INTRODUCTION. Normal liver weight 1400 - 1600g. Architecture of liver: Divided into lobules oriented around the terminal tributaries of the hepatic vein.

E N D
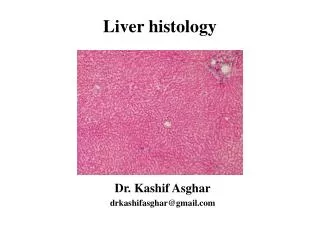
LIVER - Normal histology - Cirrhosis 8th November 2007 Dr. Cynthia Heffron Clinical Lecturer in Histopathology
INTRODUCTION • Normal liver weight 1400 - 1600g. • Architecture of liver: • Divided into lobules oriented around the terminal tributaries of the hepatic vein. • Sheets of hepatocytes with portal triads at the corner of each lobule. • Portal triad/tract: • Bile duct • Portal vein • Hepatic artery • The functional unit of the liver parenchyma is the hepatic acinus with zones 1,2 & 3. Zone 1 is periportal, zone 3 is perivenular, zone 2 intermediate.
1. Parenchyma • Liver cells (hepatocytes) trabeculae 1 cell thick in adults • Kupffer cells in sinusoids are phagocytes • Hepatic stellate cells (also called Ito cells) in space of Disse (an extrasinusoidal space) • Cells of mesenchymal origin • Store vitamin A • Transform into collagen-producing myofibroblasts when there is inflammation and fibrosis of the liver • Regulate blood flow in sinusoids • Liver-associated lymphocytes.
2. Biliary drainage system • Canaliculi (between abutting hepatocytes) • 1-2um in diameter • Canals of Hering & cholangioles • Canaliculi join to form these larger structures • Intra-hepatic bile ducts • Extra-hepatic bile ducts
3. Vasculature • Incoming blood to the liver at the porta hepatis: • Portal vein supplies 70% of the blood flow. • Hepatic artery supplies 30% of the blood flow. • Within the liver: • Sinusoids lined by fenestrated endothelium. • Blood leaving the liver: • Hepatic venules • Hepatic veins drain into the IVC.
Functions of liver • The liver is important for • Metabolism of carbohydrate, protein, lipids. • Protein synthesis, albumin, coagulation factors, complement factors etc. • Storage of iron, copper, vitamins A, D, B12. • Detoxification/drug metabolism. • Bile production.
Investigation of liver diseases • Biochemical - enzymes, proteins, bilirubin. • Haematological - coagulation factors among others. • Immunological - antibodies (viruses, autoimmune). • Imaging - ultrasound, CT, MRI, ERCP, MRCP. • Liver biopsy: • percutaneous needle biopsy, transjugular biopsy, wedge biopsy at laparoscopy or open surgery. • Useful in providing information as to the aetiology and severity of the liver disease, ruling out the presence of other concomitant disease, monitoring response to therapy. • Focal lesions require US or CT guidance.
Morphological patterns of liver injury • Degeneration • Ballooning degeneration (hydropic change) • Feathery degeneration (bile-induced damage). • Intracellular accumulations • Fat (steatosis) • Iron • Copper • Bile • Mallory’s hyaline
Haemosiderosis Mallory’s hyaline Bile Steatosis
Morphological patterns of liver injury • Degeneration • Ballooning degeneration (hydropic change) • Feathery degeneration (bile-induced damage). • Intracellular accumulations • Fat (steatosis) • Iron • Copper • Bile • Mallory’s hyaline • Necrosis • Coagulative or lytic and apoptosis. • Necrosis may be: • randomly focal (spotty necrosis), • zonal eg zone 3 • bridging (bridging hepatic necrosis, eg portal to venular), involve most or almost all of the liver (submassive and massive respectively). • Zone 3 is most prone to injury as it is farthest from the blood supply and is the area containing most drug-metabolising enzymes.
Morphological patterns of liver injury 4. Inflammation • Acute, chronic or granulomatous. • May be portal, periportal (interface hepatitis) or acinar (focal, or panacinar)
Chronic inflammation • Viral hepatitis • Granulomatous inflammation • Foreign material • Organisms • Drugs
Morphological patterns of liver injury 5. Regeneration • Hepatocytes have great ability to regenerate. • Regeneration occurs in many diseases. • Bile duct proliferation is seen in the portal tracts in cirrhosis.
6. Fibrosis • Forms in response to inflammation or direct toxic injury. • Irreversible form of liver injury. • Can be portal, perivenular, form bridging fibrosis, finally cirrhosis.
The great variety of liver diseases and the liver’s limited patterns of response means that close clinicopathological correlation is required for their diagnosis.
CIRRHOSIS • Definition: • Degenerative disease in an organ of the body, esp. the liver, marked by excess formation of connective tissue and, usually, subsequent painful swelling • Etymology: ModL < Gr kirrhos, tawny + -osis: so named by R. T. H. Laënnec (1781-1826), Fr physician, because of the orange-yellow appearance of the diseased liver • Among the top 10 causes of death in the Western world. • End stage of liver disease. • Characterised by: • Bridging fibrous septa • Parenchymal nodules • Disruption of the architecture of the entire liver
Characterised by: • Bridging fibrous septa: • Fibrosis is usually irreversible. • Regression observed rarely. • Parenchymal nodules: • Regenerative nodules surrounded by fibrosis are necessary for diagnosis. • < 3mm = Micronodular cirrhosis • Bile duct obstruction or alcohol • > 3mm = Macronodular cirrhosis • Other causes • Disruption of the architecture of the entire liver • Vasculature affected in particular with formation of abnormal interconnections between vascular inflow and hepatic vein outflow
Classification of Cirrhosis? Generally classified by Aetiology
Aetiology of Cirrhosis • Infections: • Viral hepatitis (10%). • Toxins and drugs: • Alcohol (60-70%) • Therapeutic drugs. • Autoimmune: • Hepatitis • Primary biliary cirrhosis. • Metabolic: • Haemochromatosis (5%). • Wilson disease. • Alpha-1-antitrypsin deficiency. • Glycogen storage disease and many others. • Biliary diseases (5-10%): • Congenital atresia. • Sclerosing cholangitis. • Hepatic outflow obstruction. • Cryptogenic (10-15%).
Aetiology of cirrhosis • The aetiology of cirrhosis varies throughout the world. • In the Western world, alcohol is the most common factor at 60% and viral hepatitis 10%. • Viral hepatitis is the most common factor in Asia and Africa. • Cryptogenic cirrhosis (cause unknown) forms 10%. Once cirrhosis has developed and become established, it is usually not possible to determine the aetiology by morphology alone and results of other investigations are required.
Biopsy • Used for primary diagnosis and monitoring disease. • Percutaneous, transjugular, wedge biopsies. • One study has shown that biopsy was a significant aid in establishing the diagnosis in approx 75% of cases. • Accurate interpretation of the biopsy requires clinical and laboratory data.
Mallory bodies • Characteristic of alcoholic hepatitis but not specific • Composed of tangled cytokeratin intermediate filaments and other proteins
Fatty liver Alcoholic hepatitis Cirrhosis (10-20% of alcoholics develop cirrhosis) Gross: Enlarged fatty liver Microscopic: Hepatocyte swelling and necrosis Mallory bodies Neutrophilic reaction Fibrosis Alcoholic liver disease
Individual hepatocytes are affected by viral hepatitis. • Viral hepatitis A rarely leads to signficant necrosis, but hepatitis B can result in a fulminant hepatitis with extensive necrosis. • A large pink cell undergoing "ballooning degeneration" is seen below the right arrow. • At a later stage, a dying hepatocyte is seen shrinking down to form an eosinophilic "councilman body" below the arrow on the left.
Acute Ground-glass hepatocytes (HBV) Balloon degeneration of hepatocytes Fatty change (HCV) Macrophage aggregates Apoptosis (councilman bodies, spotty necrosis) Bridging necrosis Portal tract inflammation Chronic Lymphoid aggregates Interface hepatitis Fibrosis Periportal Bridging Cirrhosis Histological features of viral hepatitis
Hereditary Haemochromatosis: autosomal recessive, chromosome 6 • Defect in intestinal absorption of iron leading to excessive absorption • Normal amount of Iron in liver – 0.5g, in haemochromatosis up to 50g • Men > women
Secondary haemochromatosis: • Most common cause = Haemolytic anaemias • Others: transfusions, alcohol • Clinically: • Main manifestations are hepatomegaly, abdominal pain, skin pigmentation, deranged glucose homeostasis or frank diabetes mellitus, cardiac dysfunction and atypical arthritis. • High risk of developing hepatocellular carcinoma.
The periportal red hyaline globules seen here with periodic acid-Schiff (PAS) stain are characteristic for alpha-1-antitrypsin (AAT) deficiency.
α1- antitrypsin (AAT) deficiency • AAT deficiency is an autosomal recessive disorder (chromosome 14) marked by abnormally low serum levels of this major protease inhibitor. • Most people with AAT deficiency are likely to develop chronic obstructive pulmonary disease with panlobular emphysema. • The globules are collections of alpha-1-antitrypsin not being excreted from hepatocytes. • This may eventually lead to chronic hepatitis and cirrhosis. • Liver disease is more likely to occur in children with AAT deficiency, while lung disease occurs in adults.
This is a case of primary biliary cirrhosis, a rare autoimmune disease. • Seen here in a portal tract is an intense chronic inflammatory infiltrate with loss of bile ductules.
Primary biliary cirrhosis • Autoimmune cholestatic liver disease mostly of middle-aged women. • Characterized by destruction of bile ductules within the triads of the liver. • This destruction is granulomatous and destroys medium sized intrahepatic bile ducts. • Antimitochondrial antibody can be detected in serum. • Micronodular cirrhosis ensues.
Pathogenesis of Cirrhosis • Liver injury results in chronic inflammation and activation of Kupffer cell, and other endogenous liver cells with the production of cytokines. • These, together with disruption of the extracellular matrix activates hepatic stellate cells (HSC). Toxins may activate HSCs. These transform into myofibroblasts which produce collagen and constrict sinusoids. • Collagen in the space of Disse leads to “capillarisation” of the sinusoids and loss of endothelial fenestrations, hindering exchange of solutes. • New vascular channels in fibrous bands link inflow of blood (venous & arterial) with outflow (hepatic venules) thus by- passing parenchyma. • Existing vascular channels and biliary channels may be obliterated. • The results are internal vascular shunts and portal hypertension. • The hepatocytes in the regenerative nodules may appear normal microscopically but are unable to adequately fulfill their functions. • Function will be further reduced if there is continuing liver cell damage.
CLINICAL FEATURES • Cirrhosis may be asymptomatic. • When symptomatic: • Non specific symptoms:weakness, fatigue, weight loss, anorexia, nausea, gaseous abdominal distension, upper abdominal discomfort. • Symptoms and signs secondary to liver failure: encephalopathy, hypoglycaemia, bleeding, ascites, overwhelming infection • Symptoms and signs secondary to portal hypertension: ascites, portosystemic venous shunts (varices), congestive splenomegaly, hepatic encephalopathy. • The liver may be enlarged, hard and irregular or smaller than normal. • Decompensated cirrhosis manifests as signs of liver failure or complications of portal hypertension. • Deterioration in liver function can be an indication of the development of hepatocellular carcinoma.
Complications of Cirrhosis • Hepatic failure • Hepatic encephalopathy • Hepatorenal syndrome • Hepatocellular carcinoma
Complications of cirrhosis (continued) 5. Portal hypertension • Portal venous pressure > 10mmHg • Causes • Prehepatic – obstructive thrombosis • Hepatic - cirrhosis • Posthepatic – right sided heart failure, constrictive pericarditis, hepatic vein outflow obstruction • Manifestations • Ascites • Transudate (<3gm/dL protein),straw coloured or pale green, a few mononuclear cells. • Risk of spontaneous infection when polymorphs predominate. • Is due to aldosterone-induced retention of Na & water, low oncotic pressure (low albumin), and portal hypertension. • Excess hepatic lymph and intestinal fluid leakage also contributes to ascites. • Portosystemic shunts • oesophageal varices • periumbilical caput medusae • haemorrhoids • Congestive splenomegaly • Hepatic encepaholopathy
Other complications due to impaired parenchymal function: • Disturbed glucose homeostasis • Impaired bile salt prodcution • Malabsortpion • Decreased albumin • Unbound drugs and metatbolites in plasma • Jaundice • Clotting factors • Oestrogen metabolism impaired • Spider naevi • Finger clubbing • Renal failure • Infections
The ultimate mechanism of most cirrhotic deaths is: • Progressive liver failure. • Complication related to portal hypertension. • Development of hepatocellular carcinoma.