Download
1 / 33
340 likes | 707 Views
Lisa Johnson, BA, SRS, LATg Certification Review Session 2010 ASR Annual Meeting Clearwater Beach, FL. Pain and Analgesia. What is Pain?. Accepted definition: An unpleasant sensory (noxious) and emotional experience associated with actual or potential tissue damage

E N D
Lisa Johnson, BA, SRS, LATg Certification Review Session 2010 ASR Annual Meeting Clearwater Beach, FL Pain and Analgesia
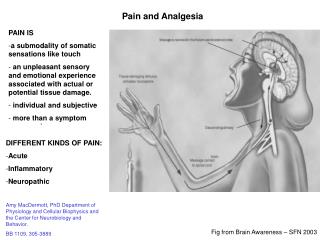
What is Pain? • Accepted definition: • An unpleasant sensory (noxious) and emotional experience associated with actual or potential tissue damage • Anything which would cause more than momentary pain in humans, should be assumed to cause pain in an animal
Definitions • Agology – the science and study of pain • Allodynia – pain caused by a stimulus that is not normally painful • Analgesia – the absence, or decrease, of pain in the presence of a stimulus that would normally be painful • Hyperalgesia – an increased sensitivity to a stimulus that is normally painful • Nociception – the reception, conduction, and central nervous processing of nerve signals resulting in the perception of pain • Somatic pain – pain originating from skin, joints, muscles, and other deep tissues • Visceral pain – pain originating from the internal organs
Definitions • Noxious stimulus – a stimulus which is actually or potentially damaging to body tissues • Pain threshold – the point at which an individual just begins to feel pain; is relatively consistent among normal individuals • Pain tolerance – the greatest amount of pain that a subject will tolerate; varies greatly among individuals • Radiculalgia – pain along the distribution of one or more sensory nerve roots • Radiculitis – an inflammation of one or more nerve roots • Wind-up – a cascade of events resulting from ongoing stimulation of nociceptors and activation of NMDA receptors; causes hyperalgesia and opioid tolerance
Types of Pain Physiological Pain Pathological Pain Results from tissue injury Inflammation occurs in the area Nerve damage Release of neurotransmitters with ongoing stimulation of nociceptors Can lead to hyperalgesia Persists after the stimulus is removed • Is a protective mechanism • Causes avoidance • Little to no tissue injury • Pain stops once the stimulus is removed
Types of Pain Acute Pain Chronic Pain Persists well past initial stimulus (3-6 months) Severity can vary May or may not respond well to treatment; may require a “multi-modal” approach Can result in allodynia, hyperalgesia, and opioid tolerance • Occurs immediately after a stimulus is received • Severity can vary • Responds well to treatment • Subsides once stimulus is removed
Physiology of Pain • Damaged cells release substances which stimulate nociceptors and inflammation • Noxious stimuli activate nociceptors, which become sensitized with stimulation, resulting in a lowered stimulation threshold • A-delta nociceptors are myelinated, conduct impulses rapidly, trigger sensation of first pain (sharp, pricking pain) • C-fibers are unmyelinated, stimulated by chemicals released in damaged or inflamed tissues, and mediates slow, burning pain
Physiology of Pain • Sensitized nociceptors cause the release of glutamate and neurokinins from the afferent terminals in the spinal cord • Activates NMDA (N-methyl-D-asparate) receptors, which are implicated in hypersensitivity (wind-up) • Afferent neurons in the spinal cord relay the signal to multiple areas in the brain, resulting in the perception of pain • “Gate control” occurs in the spinal cord, resulting in early inhibition of nociception, allowing escape
Physiology of Pain • Stimulation of medulary centers result in hyperventilation, increased cardiac output, and increased blood pressure • Descending neurons act to modulate pain by reducing sensation • Various neurotransmitters are released: glutamate, norepinephrine, serotonin, gamma-aminobutyric acid (GABA) and endorphins • Analgesia can be induced by blocking the nociceptive process at one or more points
Physiology of Pain Pain ≠ Nociception What is the difference? Pain is a product of higher brain center processing of signals it has received. Nociception refers to the peripheral and central nervous systems processing information generated by stimulation of nociceptors by noxious stimuli Nociception can occur in the absence of pain.
Physiology of Pain There are four distinct processes involved in nociception which can be modulated by analgesics: • Transduction – translation of the noxious stimulus into electrical activity at the peripheral nociceptor • Transmission – the propagation of nerve impulses through the nervous system • Modulation – modification of nociceptive transmission by inhibition of the spinal dorsal horn cells by endorphins • Perception – the final conscious subjective and emotional experience of pain
Actions of Analgesics on Pain Processes Transduction: • Can be blocked by local anesthetics by injection either at the site of injury/incision or intravenously • Can be decreased by use of NSAIDs which decrease the production of prostaglandins at the site of injury Transmission: • Can be prevented by local anesthetics by injection along peripheral nerves, at nerve plexus, or in the epidural or subarachnoid spaces Modulation: • Can be augmented by injection of local anesthetics or alpha2-adrenergic agonists; gabapentin may also effect modulation Perception: • Altered by use of general anesthetics or systemic injection of opioids and/or alpha2-agonists
Actions of Analgesics on Pain Processes • Pre-emptive analgesia: giving analgesics prior to the noxious stimulus (surgery) • By blocking or inhibiting the nociceptive process before it begins, hypersensitivity is prevented • May decrease the amount of anesthesia and post-operative analgesia needed • Multimodal or “balanced” analgesia: using a combination of analgesics which will impact more than one portion of the nociceptive process • For example: buprenorphine and meloxicam pre-surgically, lidocaine block used prior to incision, and bupivicaine splash prior to closing incision
Analgesics • Divided into five main classes based on mode of action • Opioids • Non-steroidal anti-inflammatory drugs • Local anesthetics • Alpha2-adrenoceptor agonists • Miscellaneous drugs
Analgesics - Opioids • Bind to opioid receptor sites within CNS (mostly µ but also κ) • Are agonists, partial agonists or mixed agonists-antagonists • Are controlled substances requiring special licenses and documentation of usage
Opioids • Agonists – include morphine and fentanyl • Potent opioid analgesics • Have more serious potential side effects than the mixed agonist/antagonists: respiratory depression, bradycardia, vomiting, constipation • Can be used in a continuous infusion during anesthesia • Combined with tranquilizers for neuroleptanalgesic balanced anesthesia • Can be administered intravenously, intramuscularly, via transdermal patches, and epidurally +/- local anesthetics • Can be reversed with naloxone
Opioids • Mixed agonist-antagonist – includes butorphanol • Have agonist or partial agonist activity at one or more opioid receptors and the ability to antagonize the effects of a full agonist at one or more opioid receptor • Butorphanol is a mu antagonist and kappa agonist • Butorphanol isn’t routinely used for analgesia currently due to it’s dosing frequency • Less respiratory depression than full agonists • Can be used post-operatively to reverse the narcosis of fentanyl while still providing analgesia • Has a “ceiling” effect, at which point increased doses won’t have any further effect
Opioids • Partial Agonist – includes buprenorphine • Has both agonist and antagonist activity at the mu receptor • Can be used to reverse pure mu agonists • Buprenorphine has a prolonged duration of action (relatively) • Also potential for ceiling effect
Non-steroidal Anti-inflammatory Drugs (NSAIDs) • NSAIDs are weak organic acids with anti-inflammatory, analgesic, and antipyretic properties • Inhibit prostaglandin production by inhibiting COX enzymes • Are either non-selective (inhibits both COX iso-enzymes) or selective for COX-2 • Non-selective NSAIDs have more serious side effects (gastric ulceration and renal toxicity) • Decreased renal blood flow during anesthesia makes kidneys more susceptible to toxic effects • Carprofen and meloxicam are COX-2 selective inhibitors which have a reasonable margin of safety when used pre-operatively
Local Anesthetics • Decrease or prevent Na+ permeability of the membrane of neurons, which stops the transfer of signals along the peripheral nerves • Prevent central sensitization since the nociceptive signal is blocked • Classified by duration of action • Lidocaine is short acting with a rapid on-set • Bupivicaine is long acting with a slow on-set • Duration of action can be extended by adding a vasoconstrictor like epinephrine
Local Anesthetics Multiple uses and routes of administration • Topical: most are applied to mucous membranes but some preparations will be absorbed through skin • 0.5% proparacaine is recommended for examining eyes • Lidocaine and benzocaine sprays are used to assist in intubation (benzocaine has been implicated in methemoglobinemia and should be used sparingly and with caution) • Xylocaine jell can be used to lubricate endotracheal tubes and urinary catheters • EMLA cream contains lidocaine and prilocaine and is used to numb skin
Local Anesthetics • “Splash” • Can apply to exposed tissues prior to closure and nerves prior to transection during amputations • “Soaker catheters” • Infiltration • Multiple intradermal or subcutaneous injections of local anesthetic along proposed incision line • May contain epinephrine (1:200,000) to increase effect and duration • Field block • Used to anesthetize large areas • Intradermal or SQ infiltration followed by injection deeply enough to infiltrate nerves
Local Anesthetics • Regional blocks (nerve blocks) • Injection into the connective tissue surrounding a nerve • Can produce loss of sensation and/or paralysis in the region supplied by the nerve • Requires smaller volumes than field blocks, reducing the risk of toxicity
Local Anesthetics • Epidurals • Administered alone or in combination with other analgesics • If combined, smaller doses can be used, decreasing risks of adverse effects • Can cause motor deficits at higher doses
Alpha2-Adrenergic Agonists • Stimulation of the alpha2 – adrenoceptors result in sedation, muscle relaxation, and analgesia • Can be reversed with alpha2-adrenergic antagonists such as yohimbine and atipamezole • Includes xylazine, medetomidine, and detomidine
Miscellaneous Analgesics • Tramadol • Synthetic opioid agonist which also inhibits serotonin and norepiniphrine re-uptake in the spinal cord • The main metabolite has moderate opioid activity • Ketamine • NMDA antagonist • Used as a CRI during surgery at sub-anesthetic doses, it reduces MAC and can help prevent hypersensitivity • More effective treating somatic pain than visceral pain • Can be administered via epidural injection • Gabapentin • Analogue of naturally occurring neurotransmitter GABA • Believed to increase production of GABA • Part of endogenous inhibition of nociception • Used to treat nerve pain
Pain Assessment • In order to adequately relieve pain, you need to be able to assess the presence of pain to know if your analgesic regimen is working • Need to be familiar with the species/strain you are working with to be able to recognize normal vs. abnormal behavior • Signs of pain will vary not only between various species, but between strains and individuals within a species • There is no single sign which will always indicate a specific amount of pain universally
Pain Assessment – Signs of Pain • Lethargy • Avoidance • Biting/licking at injured area • “Worried” expression • Vocalization • Disuse of limb • Aggression • Hunched posture • “Writhing” • Abnormal posture • Ruffled coat • Decreased food/water consumption • Decreased elimination • Listlessness • Hiding • “Inwardly” focused • Failure to make a nest • Disinterest in environment
Pain Assessment • Physiological changes can occur: • Increased heart rate • Increased blood pressure • Dilation of pupils • Heat in the effected area • Changes in respiration • Increased cortisol levels • Porphyrin staining around the eyes of rodents
Pain Assessment – Analog Scales • Establish parameters to score as an indicator of pain, determine what score will indicate insufficient analgesia, and have a rescue plan • Needs to be species specific • If dealing with a socialized species, can be used in conjunction with physiological parameters such as heart rate, respiratory rate, and/or blood pressure
So What Do I Need To Know? • Definitions • Types of pain • Pain pathway • Types of analgesics and their action • Pain assessment
References • Thurmon JC, Tranquilli WI, Benson GJ, eds. Lumb and Jones’ Veterinary Anesthesia, 3rd edition, Williams & Wilkins, Baltimore. 1996 • NRC, Recognition and Alleviation of Pain in Laboratory Animals, The National Academies Press, Washington, DC. 2009 • Flecknell PA and Waterman-Pearson A. Pain Management in Animals, WB Saunders, London, 2000 • Flecknell PA, Laboratory Animal Anaesthesia, 3rd edition, Academic Press, Boston, 2009