Download
1 / 42
1.64k likes | 5.9k Views
ISBAR for clear communication. Clinical communication for health employees. Aim of ISBAR education is to help you to …. further develop your communication skills utilise these skills when making a telephone referral

E N D
ISBARfor clear communication Clinical communication for health employees
Aim of ISBAR education is to help you to … • further develop your communication skills • utilise these skills when making a telephone referral • utilise questioning/prompting skills as necessary when receiving a telephone referral • standardise the use of a common agreed tool Telephone referral = any telephone conversation made by a clinician (medical, nursing, allied health) to another member of staff that relates to the immediate care of a patient
Structure of session • Introduction • Video viewing and critique (X2) • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
Why is this topic important? • Patient care is dependant on effective communication - including telephone communication between all staff involved in the care of the patient • Effective communication has become more important as healthcare has become more complex, highly specialised and team-based • JCAHO & Southern Health statistics
Why is it important to have a standard approach to telephone communication? • It is a daily task • It is rarely explicitly taught • Telephone referrals can be a source of frustration for both the ‘giver’ and the ‘receiver’ • Ineffective telephone communication can compromise patient care
Some questions for you… • How often do you make or receive a telephone referral? • Generally, is making a telephone referral easy or difficult? • What have you experienced? • If sometimes difficult, why? • What information would you like when receiving a referral?
Some of the challenges • People are busy and don’t want more work! • It can be difficult to summarise a complex case succinctly • The person making the referral • is often asked about things they have already said • may not get the help they were expecting • The person receiving the referral may • interrupt mid-sentence • make assumptions about the capability of the person making the referral
What strategies do you already use to assist the process of making or receiving a telephone referral?
ISBAR • A tool used to help provide structure to communication in a number of settings • Adapted from SBAR, a tool developed by the US Navy to improve communication • We are proposing the use of ISBAR in relation to making and receiving a telephone referral
By the end of this session you will be able to… • describe the use of the ISBAR tool in making a telephone referral • prepare for a ‘mock’ referral • demonstrate the successful use of the ISBAR tool to make a ‘mock’ referral • identify possible situations to use ISBAR in your workplace
Structure of session • Introduction • Video viewing and critique (x2) • all videos relate to the same case • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
What are your thoughts on this doctor’s attempt at making a referral?What suggestions for improvement would you give him? Video One
Focused but not prepared • The doctor clearly states what he wants • he wants the other doctor to come and see the patient • He checks he is talking to the right person but … • He doesn’t have important information at hand • The main problem is lack of preparation • how long does it take to prepare? • what things should be prepared before picking up the telephone?
What are your thoughts on this doctor’s attempt at making a referral?What suggestions for improvement would you give him? Video Two
Prepared but not focusedthis is an exaggerated vignette to make a point • The person on the other end of the phone gave up because the information was neither concise nor organised • All the relevant information was included, but … • The message was not clear Note: the relevant information needs to be delivered slowly and simply with appropriate emphasis and repetition
Structure of session • Introduction • Video viewing and critique (x2) • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
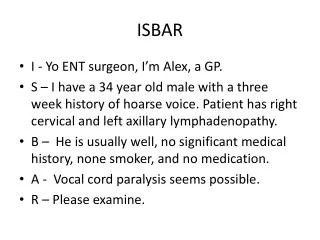
ISBAR • I - Identify • S - Situation • B - Background • A - Assessment • R - Request
ISBAR • Provides a standardised structure for communicating • Helps prioritise information for both parties • Decreases the chance of forgetting relevant information • Helps to decrease assumptions by making the reason for the call obvious at the outset
I - Identify • Identify yourself - name, position, location • Identify the person you are talking to if not already done • Identify the patient and unique ID number “Hello. My name is Jasmine Sass, I’m a Division 1 RN working on Ward 2 at …. Hospital. Are you the medical registrar on for ward referrals today? … I didn’t catch your name?…I’m calling about a patient - Terry Jones - a 56 year old man in our surgical ward at ….. Hospital”
I - Identify continued… • Why give your name? • it is polite and professional to do so • Why give your position? • helps the information receiver to know at what level to pitch their response/advice • Why state where you are calling from? • the information receiver may work at multiple sites • Why identify the person you are speaking to? • to make sure it is the appropriate person • Why do you need their name? • to document in the notes for future reference • Why identify the patient - name, age, sex, location? • helps identify the patient and helps the receiver to develop a mental picture of the patient
S - Situation • Explanation of WHY you are calling “I am calling you about a patient, Mr Jones*. He is a 56 year old man, 2 days post hernia repair who has developed new atrial fibrillation with a blood pressure of 105/66. He looks pale and feels unwell. I would like you to come and assess this patient please” • If urgent, make this clear at the start “Mr Jones is a 56 year old man who is 2 days post hernia repair. He has gone into atrial fibrillation. He is stable at present with a blood pressure of 105/66 but he is normally hypertensive. He looks pale and feels unwell. I am concerned about him and would appreciate it if you could come and help us to stabilise him” *No need to repeat patient’s name age and sex if already included in IDENTIFY
S - Situation Continued • Stating the purpose of the call at the start of the conversation helps the receiver focus their attention appropriately when listening to the story
B - Background • Tell the story “I’ll tell you the story…” “I’ll give you the background information…” • Provide RELEVANT information only. Deciding what is relevant is a skill that comes with experience • Don’t forget ‘less is often more’ • you may get the message across better with less information • Include aspects of history, examination, investigations and management where relevant
B - Background Continued… • The volume of information will depend on the situation • Less • if the receiver will see the patient themselves shortly. No background may be quite appropriate in this situation. • if the receiver already knows the patient • More • if you are wanting management advice over the phone without the receiver seeing the patient • The receiver can always fill any important gaps in your story with questions
A - Assessment • State what you think is going on. Give your interpretation of the situation • Don’t leave the receiver to guess what you are thinking - tell them • Stating the obvious is helpful here • Include your degree of certainty
A - Assessment cont… • “… the patient is febrile and I can’t find a source of infection” • “The patient has improved but I am concerned they have had a pulmonary embolus” • “The patient has acute coronary syndrome”
R - Request • State what you want from them “We would be grateful for your opinion regarding the need for surgery” “I need help urgently, are you able to come now? … If not, who should I call?” • Ask questions “What would be the most appropriate antibiotic in this situation?” “What are the priority tasks for me while you are on your way?”
Additional points… • NB: What you say for Situationmay be a concise summary of what you say for Assessment and Request. This repetition is helpful as it emphasises the key purpose of the referral • Sometimes the receiver will lead the conversation – you can still use ISBAR as a guide • Don’t forget, the receiver may not be familiar with ISBAR
Preparation for the call • Preparation is vital - use ISBAR to prepare • Make sure YOU are clear on the reason for referral before calling • Write down your questions • Document a written referral in the notes if this is the practice for formal referrals in your hospital or include in nursing notes • Gather relevant patient details, notes, charts, ECGs, observations etc before making the call • Have pen and paper on hand to write down names, numbers and instructions
Structure of session • Introduction • Video viewing and critique (x2) • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
What are your thoughts on this attempt at making a referral?This is an example of ISBAR in action… Video Three
ISBAR can be done briefly - 1 • I - “Hi, I’m Joe, an intern in ED” • S - “I would like to refer a 66 year old man with pneumonia” • B - “He has been on oral antibiotics for 1 week with no improvement. He is stable and we have commenced IV antibiotics” • A - “His presentation of pneumonia is classic” • R - “Are you able to see him with a view to admission?”
ISBAR can be done briefly - 2 • I - “Hi, I’m Sue, an ANUM on Ward 2” • S - “I would like you to come and see a 21 year old man who has had a significant skin reaction to an IV antibiotic” • B - “He was admitted this morning for treatment of an appendicectomy wound infection. He is a type 1 diabetic. He has just had his first dose of Gentamicin, Metronidazole and Ampicillin” • A - “He is anxious and appears flushed with an erythemous rash on his chest and arms. His blood pressure is normal” • R - “Are you able to see him urgently?” “What would you like me to do in the meantime?”
If you are receiving the referral • Don’t forget you can help • Are we using the ISBAR format? • Can you give this to me in ISBAR format? • Can you please identify ….? patient’s name, location • What is the Situation? • What is the Background? • What is your Assessment? • What do you think needs to happen?
Structure of session • Introduction • Video viewing and critique (x2) • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
Other applications of ISBAR • Making a written referral • Presenting a case on a ‘ward round’ • Handing over a complicated patient to covering staff • When transferring or receiving a patient from ED • ‘Standardised Forms’ development
Structure of session • Introduction • Video viewing and critique (x2) • Explanation of ISBAR tool • Video viewing and critique (x1) • ISBAR activity in pairs • Conclusion / evaluation
Conclusion ISBAR is a simple tool that enables a standardised approach to telephone referrals 7001 Medical Nursing & Allied Health staff trained at Southern Health 4760 attended sessions, 2813 evaluations completed 94.08% worthwhile,91.66% relevant to them 93.85% relevant to colleagues 38
ISBAR in Practice Diagnostic Imaging: reduction in error (Interim results - Southern Health 2009 ) Reduced inpatient misidentification: 9% to 2 % Reduced incorrect procedure verification: 30% to 4% Reduced incorrect side and site verification: 55% to 5% Referrer Audit: improved compliance. Clinical details provided 100% of time Contact details: non conformance reduced:15% to 2%
ISBAR forms • Emergency Dept to ward transfer form • Emergency surgery booking form • Medical Referral Form • Pain Consultancy Request Form New ISBAR forms discovered during evaluation • Birth Suite record of telephone contact • Wound Assessment Request
ISBAR in practice • Simulation Centre Study : Medical students assessed in SIM Centre. ISBAR trainees outperformed non trainees each time. 88% of Junior Staff using ISBAR tool six months laterMarshall et all Qual Saf Health care 2009,18(2):137-40 There is leading evidence that ISBAR promotes improved patient safety and outcomes
Questions? Thank you for supporting the use of ISBAR in our organisation ISBAR tools (2010) – developed by Southern Health in partnership with the VMIA