Download
1 / 33
330 likes | 348 Views
Learn about effective interventions to reduce disparities, current practices, and barriers in collecting race/ethnicity data in healthcare settings. Understand patient perspectives and strategies for successful data collection.

E N D
Collecting Race and Ethnicity Data: Barriers and Solutions Romana Hasnain-Wynia, PhD Health Research and Educational Trust/AHA November 3, 2006
Questions • WHY and HOWdisparities occur • Which interventions are effective at reducing or eliminating disparities • What proportion of observed disparities are amenable to improvements in health care • HOW to collect relevant data
Race/Ethnicity Data • Why Collect It • Current Practices • Barriers
Nuts and Bolts of Data Collection Addressing Discomfort Categories Staff training Start the dialogue with the community before implementing systematic data collection on race/ethnicity/language
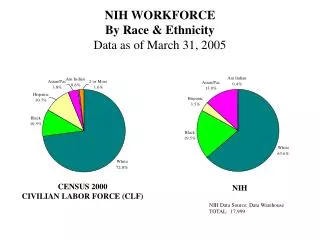
2000 Tuberculosis Rates per 100,000 population, by Race/Ethnicity and Foreign Born-Status (Newark, NJ) White Non-Hispanic 2.4 Black Non-Hispanic 21.7 Hispanic 14.8 Asian 33.2 Foreign-born 25.1 Source: Centers for Disease Control, National Center for HIV, STD, and TB Prevention
2000 Tuberculosis Rates per 100,000 population, by Race/Ethnicity and Foreign Born-Status (Jersey City, NJ) White Non-Hispanic 3.6 Black Non-Hispanic 19.8 Hispanic 12 Asian 57.3 Foreign-born 29.8 Source: Centers for Disease Control, National Center for HIV, STD, and TB Prevention
Validity and reliability of data Legal concerns System/organizational barriers Appropriate categories Patients’ perceptions/language and culture Staff discomfort in explicitly asking patients to provide this information. * Common Barriers To Collecting Data
Current Practices:National Survey of Hospitals Who, When, and How: The Current State of Race, Ethnicity, and Primary Language Data Collection in Hospitals, 2004 CMWF
Recommendations For Standardization • Who provides the information—should always be patients or their caretakers. Should never be done by observation alone • When to collect—upon admission or patient registration to ensure appropriate fields are completed when patient begins treatment • What racial and ethnic categories should be used---start with the U.S. Census categories. Hospitals can provide more”fine-grained”categories if needed • Where should data be stored—in a standard format for easy linking to clinical data • Patient Concerns—should be addressed upfront and clearly prior to obtaining information • Staff training---need to provide on-going training and evaluation
Barriers to Obtaining Race/Ethnicity Data • Concern that this will alienate patients • “Profiling” • Self-categorization (“Pick a box…”) • Use of “other” or “multiracial” categories. • Time consuming (expensive)
Most Patients Agreed That it was Important to Collect Race/Ethnicity Data “It is important for hospital and clinics to collect information from patients about their race or ethnic background? Strongly Agree 43% Somewhat Agree 37% Unsure 6% Somewhat Disagree 10% Strongly Disagree 4% Source: Baker, DW et al. “Patients Attitudes Toward Health Care Providers Collecting Information About Their Race and Ethnicity.” Journal of General Internal Medicine. 2005.
Even Stronger Support That Hospitals Should Examine Differences in Quality of Care “It is important for hospitals & clinics to conduct studies to make sure that all patients get the same high quality care regardless of their race or ethnic background.” Would you say that you: Strongly Agree 93% Somewhat Agree 4% Unsure 2% Somewhat Disagree 1%
Significant Concerns About How This Data Might Be Used How concerned would you be that this data could be used to discriminate against patients? Not concerned at all 34% A little concerned 15% Somewhat concerned 20% Very concerned 31%
Can we decrease patients’ concerns about collecting this information by providing a rationale? Four possible rationales for collecting race/ethnicity. #1 – Monitoring quality of care (“monitoring”) #2 – Mandate to collect information (“mandate”) #3 – Staff training and hiring (“needs assessment”) #4 – Possible benefits for one’s care (“personal gain”) .
Found that the “Monitoring”rationale helps patients feel the most comfortable “We want to make sure that all our patients get the best care possible, regardless of their race or ethnic background. We would like you to tell us your race or ethnic background so that we can review the treatment that all patients receive and make sure that everyone gets the highest quality of care.”
Short/Simple Version Now I would like you to tell me your Race and Ethnic Background. We use this to review the treatment patients receive and make sure everyone gets the highest quality of care.
Do Patients Like to Describe Their Race/Ethnicity in Their Own Words? • Patients asked to state race/ethnicity in terms of their choice. • Asked standard 2-part R/E questions. (OMB Categories) • Latino/Hispanic? • What is your race? (7 options read) • Asked preference between two methods
Wide Variation in Preferences for Using Own Words vs. Choosing from a List of Categories Which approach do you like better, telling your race or ethnic background using your own words or choosing from a list of categories?” Would you say that you: Strongly prefer own words 27% Somewhat prefer own words 11% Think they are about the same 30% Somewhat prefer choosing from the list 15% Strongly prefer choosing from the list 17%
Multiracial/Ethnic Individuals Strongly Preferred Using Own Words “Which approach do you like better, telling your race or ethnic background using your own words or choosing from a list of categories?” Would you say that you: Strongly prefer own words 56% Somewhat prefer own words 6% Think they are about the same 17% Somewhat prefer choosing from the list 11%
RACE QUESTION: Which category best describes your race? American Indian/Alaska Native Asian Black or African American Native Hawaiian/Other Pacific Islander White Multiracial Declined Unavailable/Unknown ETHNICITY QUESTION: Do you consider yourself Hispanic/Latino? Yes No Declined Unavailable/Unknown OMB Categories
Using OMB Categories Without Splitting Race/Ethnicity -African American/ Black -Asian -Caucasian/White -Hispanic/Latino/White -Hispanic/Latino/Black -Hispanic/Latino/Declined -Native American -Native Hawaiian/Pacific Islander -Multiracial -Declined -Unavailable/Unknown
Process Required fields Ethnicity first Ethnicity Hispanic or Latino Not Hispanic or Latino Declined Patient unavailable Preferred language [Numerous] Declined Other Patient unavailable Race American Indian or Alaskan Native Asian Black or African American Native Hawaiian or Other Pacific Islander White Multiracial: Asian/Black-African American Multiracial: Asian/White Multiracial: Black-African American/White Multiracial: Other combination Declined Patient unavailable Fields and Categories Source: Rohit Bhalla, MD, MPH Montefiore Medical Center Bronx, NY, Expecting Success Site
Conduct education and feedback sessions with leadership and staff Define issues and concerns and identify how you will respond to them Training and education components should include Policy context Revised policies New fields Screens Leadership-staff materials Staff scripts FAQs and potential answers Specific scenarios Staff questions Monitoring Systematic Implementation
In Summary • If you are just getting started, start with the basics • Collect more granular level data but develop an approach for “rolling up” granular responses to the OMB categories for analytical and reporting purposes • It can be done!
Related Publications • Hasnain-Wynia, R., Pierce, D. and Pittman, M. “Who, When and How: The Current State of Race, Ethnicity, and Primary Language Data Collection in Hospitals.” May, 2004. The Commonwealth Fund. • Baker DW, Cameron KA, Feinglass J, Georgas P, Foster S, Pierce D, Thompson J., Hasnain-Wynia R. “Patients’ Attitudes Toward Health Care Providers Collecting Information About Their Race And Ethnicity.” J Gen Intern Med. Vol 20 (10). October 2005. • Baker DW, Cameron KA, Feinglass J, Georgas P, Foster S, Pierce D, Thompson J, Hasnain-Wynia R. “Development and Testing of a System to Rapidly and Accurately Collecting Patients’ Race And Ethnicity.” Am J Public Health.Vol 96. no 3. • Hasnain-Wynia, R and Baker D.W. “Obtaining Data on Patient Race, Ethnicity, and Primary Language in Health Care Organizations: Current Challenges and Proposed Solutions.”Health Services Research (August, 2006).
Next Steps • Need to spread a clear message that providers have a key role in improving quality of care and reducing disparities • HRET is working with hospitals and ambulatory care clinics to improve race/ethnicity data collection (toolkit: www.hretdisparities.org) • HRET has trained staff at 10 hospitals to systematically collect data and link information to quality measures as part of the Robert Wood Johnson National Initiative, Expecting Success:Excellence in Cardiac Care. http://www.expectingsuccess.org/