Download

1 / 18
1.41k likes | 9.05k Views
Shoulder Dystocia. By: Sean Maclachlan & Matthew Purser. Case .

E N D
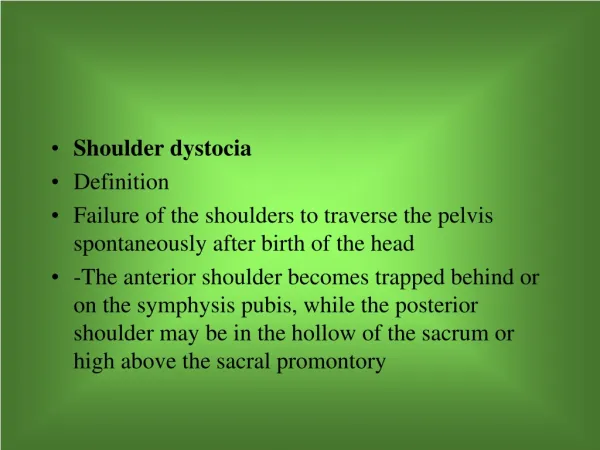
Shoulder Dystocia By: Sean Maclachlan & Matthew Purser
Case • A 30 yo G2P1 is delivering at 41 weeks gestation. She is moderately obese, but the fetus appears to clinically weigh approximately 3700 g. After a 4-hour first stage of labor and 2-hr second stage of labor, the fetal head delivers but is noted to then retract back toward the patient’s introitus (turtle sign). The fetal shoulders do not deliver, despite strong maternal pushing.
Objectives • Diagnosis of shoulder dystocia • Risk Factors of shoulder dystocia • Management principles of this obstetric emergency/ initial maneuvers to manage this condition • Review neonatal and maternal complications of this event
Diagnosis of Shoulder Dystocia Definition • Prolonged head- to-body delivery interval of > 60s as a result of the fetal ant shoulder impacting against the maternal pubic symphysis, preventing passage • Delivery of shoulder requiring the use of procedures in addition to gentle downward traction on the fetal head
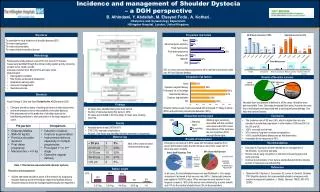
Shoulder Dystocia Incidence • 0.6-1.4% (increasing); 13-25% recurrence risk • Most cases cannot be accurately predicted or prevented Signs • Turtle Sign: appearance & retraction of the fetal head • Erythematous puffy face: indicates facial flushing from shoulder impaction within the maternal pelvis
Risk Factors Maternal Risks • Abnormal pelvic anatomy • Gestational diabetes • Previous shoulder dystocia • Short Stature Fetal Risks • Macrosomia (obesity/multiparity/DM/post-dates pregnancy) Labour Risks • Assisted Vaginal delivery (midforcepsor vacuum) – Most common risk factor • Prolonged active phase of first-stage labor • Precipitous or Protracted second stage labor *most cases are unanticipated to fetus of normal birth weight!
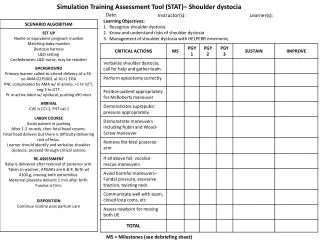
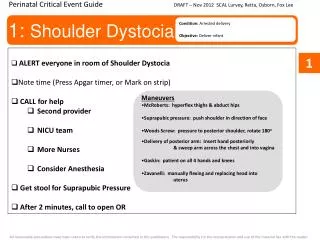
Management of Shoulder Dystocia “ALARMER”
Management of Shoulder Dystocia “ALARMER” • Apply suprapubic pressure & Ask for help • Legs - hyperflex legs (McRoberts) • Anterior shoulder dysimpaction (suprapubicpressure) • Release posterior shoulder • Maneuvreof Woods • Episiotomy • Roll onto all 4s
Management of Shoulder Dystocia McRoberts Maneuver • Sharp flexion of the legs up onto the abdomen • Tends to free anterior shoulder
Management of Shoulder Dystocia Woods “Corkscrew” Maneuver • Progressively rotate posterior shoulder 180 degrees in a corkscrew fashion, to release impacted anterior shoulder • Will deliver the posterior arm 1st
Management of Shoulder Dystocia Additional/Alternative Options • Cleidotomy: deliberate fracture of fetal clavicle • Zavanelli Maneuver – push head back into pelvis/vagina, then do emergent C/S • Symphysiotomy • Hysterotomyand subsequent vaginal delivery
Complications Maternal: Postpartum Hemorrhage (most common – 11%) • Thrid/Fourth-degree laceration • Atony – treat with uterine massage and uterotonic agents Infections • chorioamnionitis and post-partum pelvic infections Uterine rupture • abnormal thinning of the lower segment during prolonged labour Fistula – excessive pressure on tissues resulting in necrosis • vesicovaginal, vesicocervical, rectovaginal Pelvic floor/Lower extremity nerve injury • leading to prolapsy/urine or fecal incontinence Injuries subsequent to Maneuvers used: symphyseal separation, sacroiliac joint dislocation, and transient lateral femoral cutaneous neuropathy, episiotomy
Fetal: Transient Brachial Plexus Palsies (Erb-Duchenne Plexopathy) (3.0-16,8%) • Dystocia/disimpaction maneuver associated, but positioning fetus/precipitous 2nd stage/maternal forces also important + no clear fetal anthropomorphic predictor • Often resolving in 1 year with conservative therapy • Permanent palsy risk of 0.5-1.6% Clavicular Fracture (1.7-9.5%) • Typically heal without complication or need of intervention Other Fractures: Humerus (0.1-4.2%) -increased risk (20%) if delivery of posterior arm performed Hypoxic-Ischemic Encephalopathy (0.3%) • Due to cord compression Death
Clinical Pearls • Wait for a contraction after suspecting a shoulder dystocia or turtle sign. In most instances, the shoulders deliver spontaneously. • The additional 2-3 minutes on the perineum does not increase the risk of neonatal depression, acidosis, or birth asphyxia. • Use fetal maneuvers early • Avoid repeating attempts at traction, as they are likely to increase in magnitude and increase the risk for brachial plexus injury • Be aware that the McRoberts maneuver and suprapubic pressure are less effective in patients who are obese
Case • A 30 yo G2P1 is delivering at 41 weeks gestation. She is moderately obese, but the fetus appears to clinically weigh approximately 3700 g. After a 4-hour first stage of labor and 2-hr second stage of labor, the fetal head delivers but is noted to then retract back toward the patient’s introitus (turtle sign). The fetal shoulders do not deliver, despite strong maternal pushing.
Shoulder Dystocia https://www.youtube.com/watch?v=JMaAptMOSmg&list=PLrQjrSx3XGKMCtV3UZhMhQCyB9d9qaxy_ Anterior shoulder delivery http://emedicine.medscape.com/article/1602970-overview#a03
References • UpToDate – Shoulder Dystocia • Lecture Slides – Complications of Labour & Delivery: by Jenna Gale • Youtube - https://www.youtube.com/watch?v=JMaAptMOSmg&list=PLrQjrSx3XGKMCtV3UZhMhQCyB9d9qaxy_