Download
1 / 30
320 likes | 605 Views
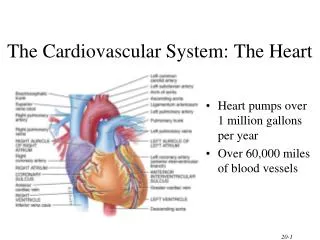
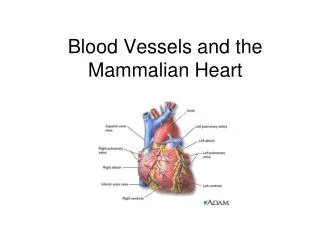
Heart & Neck Vessels—A&P . Jarvis, chapter 19. Anatomy of the Heart. Coronary Arteries. Coronary Circulation. Coronary arteries are first branches of aorta at sinuses of Valsalva. Provides blood supply to heart during diastole (during resting phase or in between beats).

E N D
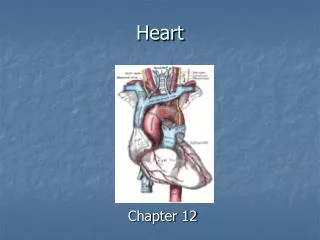
Heart & Neck Vessels—A&P Jarvis, chapter 19
Coronary Circulation • Coronary arteries are first branches of aorta at sinuses of Valsalva. • Provides blood supply to heart during diastole (during resting phase or in between beats). • Has left and right coronary branches
Left Coronary Artery • 2 branches: • Left circumflex—goes to left atrium, lateral and posterior ventricles • Left anterior descending (“widow maker”)—goes to anterior and apex of LV, anterior septum, bundle of His, right and left bundle branches
Right Coronary Artery & Venous Drainage • Goes to RA, RV, SA and AV nodes, posterior and septum • Venous drainage is done by coronary sinus, cardiac veins, and thesbian veins
Blood Flow • Realize that blood flow within the heart is bilateral • Following one deoxygenated RBC: • From body—IVC—RA—tricuspic valve—RV—pulmonic valve—pulmonary artery—lungs—pulmonary vein—LA—mitral valve—LV—aortic valve—aorta—to body
Cardiac Cycle • Systole—ventricular contraction—corresponds to “lub” sound which is closure of AV valves. This is the S1 part of cycle. • Diastole—relaxation phase and atrial contraction-- corresponds to “dub” sound which is closure of semilunar valves. This is the S2 part of cycle. • S3 is aortic valve closing just before pulmonic
So…to put it together…. • Blood from the vena cava and pulmonary artery flows into both atria when ventricles are relaxed and AV (tricuspid and mitral) valves are open. • Atria have higher pressure than ventricles so blood pours into ventricles (passive filling). • When 75% of blood is in ventricles, other 25% is pushed in by “atrial kick” (active filling). • When ventricles are full, the stretch on the chordae tendinae cause the AV valves to snap shut causing the first heart sound (S1).
And then……… • Pressure in ventricles is greater than pressure in great vessels (pulmonary artery and aorta) so… • Milliseconds later, the semilunar valves (pulmonic and aortic) open, and the ventricles contract. • Blood is forced thru the great vessels. • When pressure is low in ventricles, semilunar valves snap shut, causing the second heart sound (S2).
Preload & Afterload • Preload—amount of stretch in ventricles at end of diastole • Afterload—resistance in great vessels against which ventricles must pump blood into circulation
Cardiac Output • Cardiac output = Stroke Volume x Heart Rate • Stroke volume 70 mL/beat; 4-7 L/min; exercise 20 mL/min. SV is determined by preload, afterload, and contractility • Starling’s Law—greater the stretch, the stronger the contraction • Heart rate is controlled by ANS, CNS, and baroreceptors in heart • Ejection fraction is % of blood ejected by ventricles in one contraction
Chemical Conduction • Contraction depends on exchange of ions across the myocardial cell membrane—Na+, K+, Ca++ • Polarization—cell is ready to contract with ions in place • Depolarization—ventricular contraction • Repolarization—resting phase during which ions are moving back to polarization state
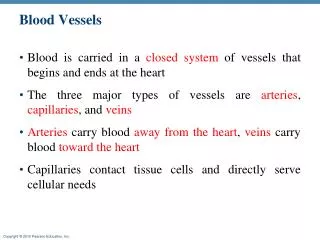
Neck Vessels (492) • Carotid artery: • Transports blood to brain • 2nd branch of aorta • Pulsations are visible • Palpated between thyroid cartilage and SCM • Coincides with apical pulse
Neck Vessels cont’d • Jugular veins: • Drain head and neck • Return blood to heart via superior vena cava (SVC) • Internal is visible in sternal notch in supine position • External may be visible superior to clavicle, but is difficult to see unless pt is in heart failure
Developmental Differences: Fetal Circulation Review • 3 anatomical differences from adult (491): • Foramen ovale—closes within 1 hr after birth • Ductus arteriosus—closes within 12-15 hrs • Ductus venosus • Blood flow differences: • Returning blood enters RA—60% goes thru foramen ovale to LA to LV, then to aorta • 40% goes to RV into PA, but only 10% goes to lungs. 30% goes to aorta
Differences: Infants and Children • PMI at 4th ICS, MCL until 7 yrs of age • Sinus arrhythmia throughout childhood • Split S2 • Faster pulse: 160 to 90 • Lower BP: 70/40 to 110/70
Differences: Older Adults • SBP increases 40 mm d/t arterial wall changes causing slight enlargement of LV. No change in DBP. • More likely to have arrhythmias, murmurs, extra sounds, bruits, activity intolerance, atypical MI sx, and orthostatic BP
Cultural Differences • All CV risk factors are higher among Blacks and Hispanics and lower in Asians and Pacific Islanders. • Incidence of HD is higher in both male and female African Americans than in other groups and Latino women have higher incidence than white women.