Download
1 / 15
160 likes | 415 Views
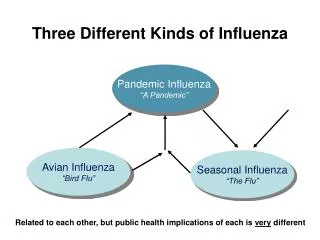
Three Different Kinds of Influenza. Pandemic Influenza “A Pandemic”. Avian Influenza “Bird Flu”. Seasonal Influenza “The Flu”. Related to each other, but public health implications of each is very different. Published Pandemic Mortality Estimates for Selected Countries

E N D
Three Different Kinds of Influenza Pandemic Influenza “A Pandemic” Avian Influenza “Bird Flu” Seasonal Influenza “The Flu” Related to each other, but public health implications of each is very different
Published Pandemic Mortality Estimates for Selected Countries (Johnson NPAS & Mueller J. Bulletin of the History of Medicine (2002) 76:105-15) (1918: 28% of current global population. http://birdfluexposed.com/resources/NIALL105.pdf) British isles: 249,000 Russia/USSR: 450,000 Canada: 50,000 Japan: 388,000 Afghan.: 320,000 Spain: 257,000 USA: 675,000 Egypt: 139,000 Philip.: 94,000 Bangl./ India/ Pak.: 18.5 million Guatemala: 49,000 Nigeria: 455,000 Kenya: 150,000 Indonesia: 1.5 million Brazil: 180,000 Australia: 15,000, in 1919 only South Africa: 300,000 Chile: 35,000 Global Total: 50 – 100 million (WHO: 40 million +) Sequestration completely protected American Samoa, & Australia from the 2nd wave, while Western Samoa lost 22% of its population
“In Philadelphia the number of dead quickly overwhelmed the city’s ability to handle bodies. It was forced to bury people, without coffins, in mass graves and soon began using steam shovels to dig the graves.” (John Barry, The Great Influenza)
Origin of Pandemic Influenza (All human flu pandemics come from bird flu by 1 of 2 mechanisms) Migratory water birds H 1-16 Domestic pig N 1-9 Domestic birds
H5N1’s Global Genetic Roulette Table Persistence & spread of H5N1 is historically unprecedented for HPAI (61 countries)
Continuing Widespread H5N1 HPAI = ContinuingSerious Pandemic Threat Less H5N1 HPAI in wild migratory birds in 2007/2008 than in 2006 H5N1 HPAI in poultry is now endemic in several countries, including Bangladesh, Egypt, Indonesia, & Viet Nam. (28 countries in 2007)
Expect human cases in all areas with substantial human exposure to HPAI H5N1+ birds Expect human cases in all areas with substantial human exposure to H5N1 HPAI+ birds As of June 17, 2008: 383 lab.-confirmed cases in 15 countries,including 241 deaths (Case Fatality: `63%)
H5N1 in 1997 & Since 2003: Three Requirements for a Flu Pandemic: • Novel flu virus for humans Yes • Ability to replicate in humans Yes& cause illness • Ability to pass easilyNot Yetfrom person to person (signaled by growing clusters / outbreaks of human cases)
WHO phases apply to the whole world. Phases 4 & 5 may be skipped
Modes of Person-to-Person Transmission: Close Exposure (maximum2 meters / 6 feet): • Large droplets from coughing, sneezing, & talking, to other’s eyes, nose, or mouth; • Contact: direct(hand-to-hand) & indirect (hand-to-surface-to-hand – less common?); • ? Airborne / aerosol / droplet nuclei: By aerosol-generating medical procedures & in shared air spaces with poor air circulation? Can remain suspended in air for longer, but NOT long distance or in ventilation systems? Courtesy of CDC
1918, 1957, & 1968 US & UKOverall Clinical Attack Rates Range: ~ 23% – 39%. (Slide from Dep. of Health, National Health Service, UK)
In Connecticut “local health departments ….. currently note, somewhat incredulously, that, in the event of Pandemic Flu, they are responsible for: • “Community quarantine & isolation ....... ; • “Instituting ….. social distancing ……… ; • “Mass Care, i.e., taking care of those too ill to be at home ….. when the hospitals have exhausted surge capacity & shut their doors; • “Mass Fatalities, i.e., collecting large numbers of bodies when the ordinary medical examiner & mortuary processes have collapsed; • …… “without any assistance from any outside source, as it is assumed that every community is undergoing the same crisis.” (From a local health department in Connecticut, Feb. 2007)
Pandemic Wave Peak Worker-Absenteeism ~50% (?)+ Long Supply Lines & Just-In-Time Delivery of Goods = Big Impact on Availability of Goods & Services?
CATEGORIES OF RISK – AVIAN & PANDEMIC INFLUENZA UNSIC Livelihoods • Food & income loss from poultry deaths, culling & decreased economic activity • High illness & potentially high death rates • Overstretched health facilities • Disproportionate impact on vulnerable Human Health • Increased demand for governance & security • Higher public anxiety • Reduced capacity due to illness & death Governance & Security • Deterioration of coping & support mechanisms • Interruption in public services • Quarantine policies Social & Humanitarian Needs • Trade & commerce disruptions • Degraded labour force • Interruption of regular supply systems Economic Systems
Conclusions (1)Key Unpredictables • Will it come from H5N1 or from another subtype? • Will we move from Phase 3 to Phase 6 overnight or over months? • Will it hit next week, next year, or next decade? • What roles will immunization & anti-virals play? • How high will mortality be? (1968, 1918, ~H5N1?) • How much economic & social disruption?