Download
1 / 1
10 likes | 171 Views
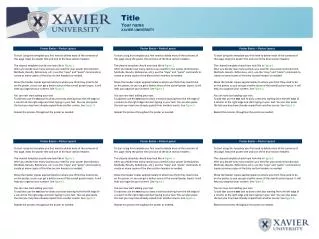
Trends in Antimicrobial Susceptibility of Bacterial Pathogens Isolated from Patients with Blood Stream Infections (BSI) in North America (NA): SENTRY Program, 1997-2000. 1997 Rank Pathogen No. (%) a 1 S. aureus 1802 (22.9) 2 E. coli 1461 (18.6) 3 CoNS 1008 (12.8)

E N D
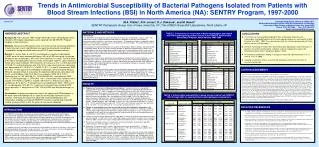
Trends in Antimicrobial Susceptibility of Bacterial Pathogens Isolated from Patients with Blood Stream Infections (BSI) in North America (NA): SENTRY Program, 1997-2000 1997 Rank Pathogen No. (%)a 1 S. aureus1802 (22.9) 2 E. coli1461 (18.6) 3 CoNS 1008 (12.8) 4 Enterococcus spp. 745 (9.5) 5 Klebsiella spp. 592 (7.5) 6 S. pneumoniae441 (5.6) 7 P. aeruginosa359 (4.6) 8 Enterobacter spp. 312 (4.0) 9 -streptococcus 277 (3.5) 10 viridans group streptococci 120 (1.5) 1998 Rank Pathogen No. (%)b 1 S. aureus 1683 (24.5) 2 E. coli 1183 (17.2) 3 CoNS 879 (12.8) 4 Enterococcus spp. 721 (10.5) 5 Klebsiella spp. 518 (7.5) 6 S. pneumoniae 345 (5.0) 7 P. aeruginosa 306 (4.4) 8 -streptococcus 239 (3.5) 9 Enterobacter spp. 230 (3.3) 10 viridans group streptococci 120 (1.7) S. aureus CoNS Enterococcus spp. S. pneumoniae E. coli Klebsiella spp. P. aeruginosa Enterobacter spp. Oxacillin Oxacillin Vancomycin PenicillinLevofloxacin CeftazidimeCefepimeCiprofloxacin CeftazidimeCefepime CeftazidimeCefepimeImipenemCiprofloxacin CeftazidimeCefepime 77.6 (1802) 29.9 (1008) 87.0 (745) 65.8 (441) 99.3 (441) 99.2 (1461) 99.9 (1461) 97.5 (1461) 96.3 (592) 98.8 (592) 86.9 (359) 88.3 (359) 87.5 (359) 88.9 (359) 77.9 (312) 100.0 (319) 72.2 (1683) 23.2 (879) 86.4 (721) 81.2 (345) 99.7 (345) 98.6 (1183) 99.7 (1183) 97.4 (1183) 95.4 (518) 99.4 (518) 83.0 (306) 87.9 (306) 91.8 (306) 85.9 (306) 75.2 (230) 99.1 (230) 69.3 (1945) 25.6 (935) 85.4 (763) 78.2 (349) NA 99.4 (1315) 99.8 (1315) 95.4 (1315) 96.3 (597) 98.8 (597) 85.1 (335) 88.1 (335) 90.7 (335) 85.4 (335) 77.7 (287) 99.0 (287) 65.6 (1917) 23.7 (739) 84.2 (703) 78.2 (261) 100.0 (261) 99.0 (1118) 100.0 (1118) 95.3 (1118) 96.4 (494) 99.6 (494) 88.2 (306) 89.5 (306) 92.2 (306) 78.8 (306) 81.2 (239) 99.2 (239) M.A. Pfaller1, R.N. Jones2, D.J. Diekema2, and M. Beach2SENTRY Participants Group. Univ of Iowa, Iowa City, IA1; The JONES Group/JMI Laboratories, North Liberty, IA2 Poster # 78 • *Corresponding Author: Michael A. Pfaller, M.D. • Medical Microbiology Division, C606 GH, Department of Pathology • University of Iowa College of Medicine, Iowa City, Iowa 52242 • Phone: (319) 384-9566 Fax: (319) 356-4916 • Email: michael-pfaller@uiowa.edu • CONCLUSIONS • In summary, we have provided longitudinal data on pathogen frequency and antimicrobial susceptibility profiles of the most important organisms causing BSI in North America from 1997 - 2000. These data demonstrate the increasing prominence of Gram-positive cocci as BSI pathogens. • Likewise, increasing resistance was observed among staphylococci and enterococci. In contrast, the activity of ceftazidime, cefepime, and the carbapenems against the Enterobacteriaceae and P. aeruginosa appears stable. • Resistance to ciprofloxacin among P. aeruginosa increased significantly from 7.5% in 1997 to 17.3% in 2000. • Ongoing surveillance remains essential and should be used to limit the extent of resistance world-wide. AMENDED ABSTRACT Background: From January 1997 through December 2000, 29,052 blood stream infections (BSI) bacterial pathogens were reported from 38 SENTRY Program hospitals in North America. Methods: Consecutive BSI isolates were sent to the central monitoring laboratory in Iowa City each month. Identification was confirmed and broth microdilution susceptibility testing was performed using NCCLS recommended methods. Results:S. aureus (SA), E. coli (EC) and coagulase-negative staphylococci (CoNS) were the most common pathogens; 55% of all BSI during the 4-yr period. Among the top 10 pathogens, 63% were Gram-positive (G+) cocci. The rank order of the top 10 BSI pathogens was essentially unchanged; however, some important trends were noted. Between 1997 and 2000, an increase in the % of BSI due to SA (22.9-28.7%) and Enterococcus spp. (9.5-10.5%) was noted, whereas a decrease was observed for EC (18.6-16.7%), CoNS (12.8-11.1%) and S. pneumoniae (SPN; 5.6-4.6%). 16 key organism-antimicrobial combinations were evaluated (NCCLS MICs) for possible trends in resistance. No significant differences were observed for EC vs ceftazidime (CAZ; 99.2-99.0%) or cefepime (CPM; 99.9-100%); Klebsiella spp. vs CAZ (96.3-96.4%), CPM (98.8-99.6%), and imipenem (IMP; 100%); Enterobacter spp. vs CPM (99.0-100%). Decreased S was noted for SA vs oxacillin (77.6-65.6%); CoNS vs oxacillin (29.9-23.7%); Enterococcus spp. vs vancomycin (87.0-84.2%); P. aeruginosa versus ciprofloxacin (88.9 - 78.8%) and EC vs ciprofloxacin (97.5-95.2%). In contrast, increased S was noted for SPN versus penicillin; P. aeruginosa vs CPM, CAZ and IMP and Enterobacter spp. vs CAZ. Conclusions: Important changes over time in the spectrum of BSI pathogens in NA were noted and highlight the G+ cocci as increasingly significant causes. Likewise, increasing resistance was observed among staphylococci and enterococci. Ongoing surveillance (SENTRY) remains essential and should be used to enhance efforts to limit the extent of resistance worldwide. MATERIALS AND METHODS TABLE 1. Frequencies of occurrence of bacterial pathogens associated with BSI in participating medical centers in the SENTRY Antimicrobial Surveillance Program, North America 1997-2000 Study Design The SENTRY Antimicrobial Resistance Surveillance Program was established in January 1997. The monitored infections include bacteremia and fungemia, outpatient respiratory tract infections, pneumonia, wound infections, and urinary tract infections. Participating institutions include 30 medical centers in the US, eight in Canada, ten in Latin America, and 24 in Europe. This report will focus on all BSI isolates from the North America. Each participant hospital contributed results (organism identification, date of isolation, and antimicrobial susceptibility profile) on the first 20 consecutive episodes of bacteremia (blood culture isolates from separate patients that were judged to be clinically significant) in each calendar month of each year. All isolates were saved on agar slants and sent on a weekly basis to the University of Iowa (Iowa City) for storage and for further characterization by reference identification and susceptibility testing methods. Organism Identification All blood culture isolates were identified at the participating institution by the routine methods in use at each laboratory. Upon receipt at the University of Iowa, isolates were subcultured to blood agar to ensure viability and purity. Confirmation of species identification was performed with Vitek (bioMerieux Vitek, St. Louis, MO) and API (bioMerieux) products or conventional methods as required. Isolates were frozen at -70C until needed. Susceptibility Testing Antimicrobial susceptibility testing of isolates was performed by reference broth microdilution methods as described by the National Committee for Clinical Laboratory Standards. Microdilution trays were purchased from Accumed, Inc. (Cleveland, OH). Quality control was performed by testing E. coli ATCC 25922, S. aureus ATCC 29213, P. aeruginosa ATCC 27853, S. pneumoniae ATCC 49619, and Enterococcus faecalis ATCC 29212. Interpretive criteria for each antimicrobial agent tested were those published by NCCLS. • aPercent of 7,854 isolates • bPercent of 6,878 isolates 1999 Rank Pathogen No. (%)c 1 S. aureus1945 (25.5) 2 E. coli1315 (17.2) 3 CoNS 935 (12.2) 4 Enterococcus spp. 763 (10.0) 5 Klebsiella spp. 597 (7.8) 6 S. pneumoniae349 (4.6) 7 P. aeruginosa335 (4.4) 8 Enterobacter spp. 287 (3.8) 9 -streptococcus 279 (3.7) 10 Serratia spp. 136 (1.8) 2000 Rank Pathogen No. (%)d 1 S. aureus1917 (28.7) 2 E. coli1118 (16.7) 3 CoNS 739 (11.1) 4 Enterococcus spp. 703 (10.5) 5 Klebsiella spp. 494 (7.4) 6 P. aeruginosa306 (4.6) 7 S. pneumoniae261 (3.9) 8 Enterobacter spp. 239 (3.6) 9 -streptococcus 234 (3.5) 10 Serratia spp. 102 (1.5) ACKNOWLEDGEMENTS The authors wish to thank K. Meyer for her assistance in the preparation of this manuscript. The authors express their appreciation to all SENTRY site participants. Participants contributing data/isolates to the study included: The Medical Center of Delaware, Wilmington, DE, (L. Steele-Moore); Clarion Health Methodist Hospital, Indianapolis, IN, (G. Denys); Henry Ford Hospital, (C. Staley); Summa Health System, Akron, OH (J.R. Dipersio); Good Samaritan Regional Medical Center, (M. Saubolle); Denver General Hospital, Denver, CO, (M.L. Wilson); University of New Mexico Hospital, Albuquerque, NM, (G.D. Overturf); University of Illinois at Chicago, Chicago, IL, (P.C. Schreckenberger); University of Iowa Hospitals and Clinics, Iowa City, IA, (R.N. Jones); Creighton University, Omaha, NE, (S. Cavalieri); Froedtert Memorial Lutheran Hospital-East, Milwaukee, WI, (S. Kehl); Boston VAMC, Boston, MA (S. Brecher); Columbia Presbyterian Medical Center, New York, NY, (P. Della-Latta); Long Island Jewish Medical Center, New Hyde Park, NY, (H. Isenberg); Strong Memorial Hospital, Rochester, NY, (D. Hardy); Kaiser Regional Laboratory, Berkeley, CA, (J. Fusco); Sacred Heart Medical Center, Spokane, WA, (M. Hoffmann); University of Washington Medical Center, Seattle, WA, (S. Swanzy); Barnes-Jewish Hospital, St. Louis, MO, (P.R. Murray); Parkland Health & Hospital System, Dallas, TX, (P. Southern); The University of Texas Medical School, Houston, TX, (A. Wanger); University of Texas Medical Branch at Galveston, Galveston, TX (B. Reisner); University of Louisville Hospital, Louisville, KY, (J. Snyder); University of Mississippi Medical Center, Jackson, MS, (J. Humphries); Carolinas Medical Center, Charlotte, NC, (S. Jenkins); University of Virginia Medical Center, Charlottesville, VA, (K. Hazen); University of Alberta Hospital, Edmonton, Alberta, CAN,( R. Rennie); Health Sciences Centre, Winnipeg, Manitoba, CAN, ( D. Hoban); Queen Elizabeth II Health Sciences Centre, Halifax, Nova Scotia,CAN, (K. Forward); Ottawa General Hospital, Ottawa, Ontario, CAN, (B. Toye); Royal Victoria Hospital, Montreal, Quebec, CAN, (H. Robson); Microbiology Laboratory C.E.M.I.C., This study was supported by a research and educational grant from Bristol-Myers Squibb Company. RESULTS • Frequency of occurrence of bloodstream pathogens. During the four year study period, (January 1997 through December 2000), a total of 29,052 BSI were reported by North American SENTRY participants. Table 1 compares the frequencies of occurrence of the 10 most commonly isolated pathogens during each of the four years, 1997-2000. These organisms and groups accounted for 91% of all BSI reported from these hospitals during the four year period. The rank order of the top five pathogens was unchanged from 1997 to 2000. These five organisms or organism groups (Staphylococcus aureus, Escherichia coli, coagulase-negative staphylococci, Enterococcus spp. and Klebsiella spp.) accounted for over 70% of all BSI during the four sampling periods. Notably, between 1997 and 2000, an increase in the percentage of BSI due to S. aureus (22.9 - 28.7%) and Enterococcus spp. (9.5 - 10.5%) was seen, whereas a decrease was observed for E. coli (18.6 - 16.7%), CoNS (12.8 - 11.1%) and S. pneumoniae (5.6 - 4.6%). • Change in susceptibility over time for selected antimicrobial-pathogen combinations, by region. In order to follow changes in important antimicrobial resistances, we selected a number of sentinel antimicrobial-organism combinations (adapted from Archibald, et al.(12). A comparison of susceptibility results over the four year period was made for each of these antimicrobial-organism combinations in each region (see Table 2). • Oxacillin resistance among Staphylococcus spp. (both S. aureus and CoNS) increased over the four year time period. In 1997, 22.4% of S. aureus BSI isolates were oxacillin-resistant; this increased to 34.4% by 2000. Oxacillin-resistance among CoNS increased from 70.1% in 1997 to 76.3% in 2000. • There was a moderate increase in vancomycin-resistance among the Enterococcus spp. BSI isolates between 1997 and 2000: 11.5% to 14.5%. • Among the S. pneumoniae BSI isolates, high level resistance to penicillin (MIC, 2 g/ml) decreased from 9.4% in 1997 to 7.6% in 2000. Likewise, ~ 99% of S. pneumoniae isolates were susceptible to levofloxacin over the four year study period. • Among the four most prevalent causes of gram-negative BSI, no increase in resistance to cefepime or the carbapenems was seen between 1997 and 2000. Susceptibility to ceftazidime increased by 1 - 6% among isolates of Klebsiella spp., P. aeruginosa, and Enterobacter spp. Ciprofloxacin activity against E. coli BSI decreased slightly from 97.5% susceptible in 1997 to 95.2% in 2000. Importantly, ciprofloxacin activity against P. aeruginosa decreased by approximately 10% (88.9-78.8%) between 1997 and 2000. • cPercent of 7,635 isolates • dPercent of 6,685 isolates TABLE 2. Antimicrobial susceptibility in blood stream isolates from SENTRY 1997 through 2000 for selected antimicrobial-pathogen combinations Organism Antimicrobial Agent % Susceptible(No. Tested) 1997 1998 1999 2000 SELECTED REFERENCES INTRODUCTION • 1. Archibald L, Phillips D, Monnet JE, McGowan JE, Tenover F, and Gaynes R. Antimicrobial resistance in isolates from inpatients and outpatients in the United States: increasing importance of the intensive care unit. Clin. Infect. Dis. 1997;24:211-215. • 2. National Committee for Clinical Laboratory Standards. Methods for dilution antimicrobial tests for bacteria that grow aerobically. Approved standard M7-A4, National Committee for Clinical Laboratory Standards, Wayne, PA, 1997. • 3. National Committee for Clinical Laboratory Standards. Performance standards for antimicrobial susceptibility testing. Supplemental tables M100-S8., National Committee for Clinical Laboratory Standards, Wayne, PA, 1998. • 4. Pfaller MA, Jones RN, Doern GV, Kugler K, et al. Bacterial pathogens isolated from patients with bloodstream infection: Frequencies of occurrence and antimicrobial susceptibility patterns from the SENTRY antimicrobial surveillance program (United States and Canada, 1997). Antimicrob. Agents Chemother. 1998;42:1762-1770. • 5. Pfaller MA, Jones RN, Doern GV, Sader HS, Kugler K, Beach M, et al. Survey of bloodstream infections due to Gram-positive cocci: Frequency of occurrence and antimicrobial susceptibility of isolates collected in 1997 in the United States, Canada, and Latin America for the SENTRY antimicrobial surveillance program. Diagn. Microbiol. Infect. Dis. 1999;33:283-297. • 6. Pittet D, Li N, Woolson RF, and Wenzel RP. Microbiological factors influencing the outcome of nosocomial bloodstream infections: a 6-year validated, population-based model. Clin. Infect. Dis. 1997;24:1068-1078. • 7. Weinstein MP, Towns ML, Quartey SM, et. al. The clinical significance of positive blood cultures in the 1990’s: A prospective comprehensive evaluation of the microbiology, epidemiology and outcome of bacteremia and fungemia in adults. Clin. Infect. Dis. 1997;21:584-602. The SENTRY antimicrobial resistance surveillance program is designed to track antimicrobial resistance trends nationally and internationally through a network of sentinel hospitals. Previous publications from SENTRY have established baseline data regarding the spectrum of pathogens and antimicrobial resistance profiles of organisms causing bloodstream, respiratory tract, wound, and urinary tract infections in North and Latin America. These data demonstrate significant regional differences in antimicrobial susceptibility and confirm the widespread nature and alarming prevalence of antimicrobial resistance in the Western Hemisphere. It is important not only to establish the prevalence of antimicrobial resistance at one point in time, but to provide longitudinal data to track changes over time. The rates of change in resistance by pathogen and region can help set priorities for focused intervention efforts. Bloodstream infections (BSI) cause significant morbidity and mortality worldwide. In this paper we report the frequencies of occurrence and antimicrobial susceptibility profiles of bloodstream infection (BSI) isolates from the North America medical centers participating in the SENTRY program. The present study included all BSI from January 1997 through December 2000. A156-34