Download
1 / 28
280 likes | 427 Views
Prevention and Early Intervention (PEI) Guidelines Webcasts. Building Partnerships: Strategies for Outreach and Engagement to Underserved Ethnic and Cultural Communities in Your County. DMH/CRHD Interagency Agreement Center for Reducing Health Disparities UC Davis School of Medicine

E N D
Prevention and Early Intervention (PEI) Guidelines Webcasts Building Partnerships: Strategies for Outreach and Engagement to Underserved Ethnic and Cultural Communities in Your County DMH/CRHD Interagency Agreement Center for Reducing Health Disparities UC Davis School of Medicine November 2, 2007
Context • The MHSA calls for an expansion of mental health services with a focus on underserved and unserved populations • The PEI Guidelines have identified: • Disparities in access to mental health services as a key community need • Underserved and unserved communities as key populations • A Community Program Planning Process that requires outreach and engagement to underserved and unserved communities
PEI Guidelines • “Efforts should be made to include individuals from underserved racial/ethnic and cultural communities in the planning process.” • “Outreach efforts could include consultations with key informants, members and leaders of underserved communities with knowledge of mental health needs.” • “Input from key informants could be sought through focus groups and other appropriate methods regarding community perceptions of needs, priority populations, community assets relevant to PEI efforts, potential projects and evaluation methods.” Source: http://www.dmh.ca.gov/DMHDocs/default.asp?view=notices, p. 14
PEI Guidelines • “These efforts might have as their goal the ongoing inclusion of community perspectives in PEI component implementation over the long term.” • “Informants representing underserved communities should be involved in the drafting of county components.” • “Successful outreach and engagement processes in the planning stage can be reflected in elements of the county components, demonstrating collaboration with community based organizations to address needs of underserved communities.” Source: http://www.dmh.ca.gov/DMHDocs/default.asp?view=notices, p. 14
“Go in search of people. Begin with what they know. Build on what they have” Chinese proverb
Release of the UCD CRHD-DMH ReportBUILDING PARTNERSHIPS:KEY CONSIDERATIONS WHEN ENGAGING UNDERSERVED COMMUNITIES UNDER THE MHSA Purpose of the Report: Introduce guiding principles of community engagement with underserved communities; Outline some guiding questions to assist counties in their MHSA community outreach and stakeholder processes; Suggest specific strategies that Counties Mental Health departments might employ to nurture sustained and equitable partnerships with communities.
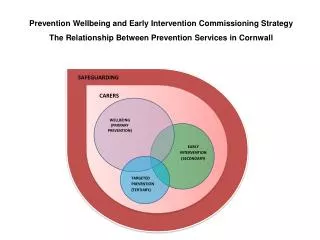
CRHD Recommended Strategies • Identifying underserved communities within your county • Establishing bi-directional relationships • Finding community representatives • Facilitating meetings and exchanging information • Engaging community representatives and maximizing the opportunity for trusting communication • Using the information once it is collected • Making sure the voices are heard and integrated into PEI programmatic plans • Building ongoing partnerships
1. Identifying Underserved Communities Within your County Groups historically underserved by mental health services Groups facing geographic or linguistic barriers to care PEI priority populations Local priority populations Groups with high uninsurance, underinsurance and/or poverty rates
1. Identifying Underserved Communities Within your County (cont’d) • Tap into data sources • Census data • Statewide and local reports • California Health Interview Survey (CHIS) • Kaiser Family Foundation • The California Endowment • Public School data • First 5 Children and Families Commission data • Trends of penetration rates • Department of Public Health data • Data resources within communities such as United Way, NGOs, etc.
2. Establishing Bi-directional Relationships • Clarity of purpose • Understand that the relationship will be a two-way relationship • Awareness of past interactions with community • Recognize that part of the purpose is building up ongoing relationships • Be clear about how participants can influence the decisions that may be made and what issues cannot be influenced
2. Establishing Bi-directional Relationships (cont’d) • Understanding the partner community • Be clear about who should be engaged • Identify the community leaders and key community organizations with whom to partner (who has trust, respect, and credibility within the community?) • Address the “culture”, as well as the cultural, language, racial, and ethnic issues of the community • Use awareness and sensitivity when working with tribal communities. Recognize and honor tribal sovereignty issues
2. Establishing Bi-directional Relationships (cont’d) • Approach communities with awareness of past interactions with community and be prepared to address mistrust and disbelief • Be aware of how government agencies are perceived • Validate concerns • Be transparent about your purpose and reasons for being there
2. Establishing Bi-directional Relationships (cont’d) • Identify opportunities for co-learning • From the community to the county: the communities’ needs, priorities, assets, existing resources • Existing services, programs that can be enhanced or supported by PEI initiative • From the county to the community: Informing opportunities for accessing funds and learn about procurement process and participation in policy decisions
3. Facilitating Meetings and Exchange of Information • In your initial communications with the community, be clear about your financial, time, personnel and other constraints • Approach the community cultural brokers for advice on • Who to talk with (e.g., men and women separately?, immigrants by how long they have been here, by ethnic subgroup) • Where to hold meetings (e.g., schools, community centers, migrant camps) • When to hold meetings (e.g., evenings on weekdays, weekday during the day, or weekend afternoons)
3. Facilitating Meetings and Exchanging Information (cont’d) • Approach the community cultural brokers for advice on • Who should facilitate the meeting: Is ethnic, cultural, and language matching important? • Should the facilitator be a member of the community or a county representative? • How questions should be worded?
3. Facilitating Meetings and Exchanging Information (cont’d) • Choice of methodology • Focus groups (8-10 people) • Community/town forums (e.g., 50+ people, open to the public) • Face-to-face interviews (with “key” community members) • Surveys: face-to-face with interviewer or self-administered written survey
3. Facilitating Meetings and Exchanging Information (cont’d) • Tips on running focus groups • Facilitator should have a good understanding of PEI guidelines, the purpose of community participation, and know how to promote a safe and trusting environment for the discussion • Consider employing health outreach workers already experienced with the community (e.g., promotores/as) • Come in with broad themes and have the flexibility to let the community set the direction of discussion
3. Facilitating Meetings and Exchanging Information (cont’d) • Tips on running focus groups • Determine most reliable way to capture the information (e.g., multiple note takers, audio recording, facilitator summarizing points on paper visible to audience, use of LCD projector) • Immediately after the focus group is complete, facilitator or other county participant should write a summary of the content • If interpreters are to be used, allocate enough resources to have experienced interpreters at hand
3. Facilitating Meetings and Exchanging Information (cont’d) • Tips on conducting surveys • Keep it simple; it is best if written surveys take no more than 15 minutes to complete • Pre-test questions on a small number (e.g., 10) of people from the partner community; speak to them afterwards to get their feedback about the questions (e.g., did they make sense?) • The best questions are ones that elicit a variety of responses; but not too much variety
3. Facilitating Meetings and Exchanging Information (cont’d) • Translations and Adaptations • This should not be an afterthought • Allocate enough resources and time for quality translations and adaptations of written materials; the translations and adaptations must address both language and cultural content • Utilize assets within the partner community and/or public health/school-based organizations • Review of materials should be done in collaboration with community cultural brokers and qualified bilingual county staff
4. Using the Information Once it’s Available Focus group, townhall/community meetings, one-on-one interviews • Issues to consider • Transcription: Consider transcription of agreed upon key parts only • One suggestion: Have facilitator write summary of content and two others independently review audio/transcription and independently write summaries • Compare the summaries, resolve differences, and merge into a single summary
4. Using the Information Once it’s Available (cont’d) • Making sure the voices are heard and integrated into plans • Translating community input into the PEI plan for counties • Community program planning process
Suggestions Emerging for MHSA PEI Planning Process • Engage underserved communities in places that matter to them (e.g., ESL classes, housing assistance, social service agencies); • Consider the role of paraprofessionals; • Integrate mental health outreach and treatment with other health and social services.
Strengthening Counties’ Community Input Process • Limited time or capacity to address all the communities in the state that have specific needs. • How can counties make community outreach and engagement an integral part of ongoing policy processes? • Outreach takes time and long-term investment in communication and building trust. • How can counties maintain ongoing relationships of trust with underserved communities over time?
Selected Sources • US Census Bureau: • American Community Survey: Data Profiles 2003 for Californiahttp://www.census.gov/acs/www/Products/Profiles/Single/2003/ACS/CA.htm • Centers for Disease Control and Prevention: • Principles of Community Engagement: http://www.cdc.gov/phppo/pce/ • The Kaiser Family Foundation: • The Uninsured and their Access to Health care:http://www.kff.org/uninsured/upload/1420_09.pdf • The California Endowment: • Health Coverage Expansion in California: What Can Consumers Afford to Spend?:http://www.calendow.org/uploadedFiles/Health_Expansion_PB_091807(1).pdf
Selected Sources (cont’d) • Institute of Medicine of the National Academies: • Reports on Uninsurance: http://www.iom.edu/CMS/3809/4660/4662.aspx • Coverage Matters: Insurance and Health Care: http://www.nap.edu/catalog.php?record_id=10188 • United Way: • Racial and Ethnic Health Disparities: A Review of Selected State Programs: http://www.library.ca.gov/crb/06/02/06-002.pdf • California Health Interview Survey: http://www.chis.ucla.edu • UCLA Center for Policy Research: • Health Insurance Coverage and Programs: http://www.healthpolicy.ucla.edu/pubs/pubList.asp?topicID=5 • Barriers to Disparities in Health Care: http://www.healthpolicy.ucla.edu/pubs/pubList.asp?topicID=1&subTopicID=1
Selected Sources • First 5 California – have done asset mapping • http://www.ccfc.ca.gov/ • Department of Social Services – information on foster care services • http://www.cdss.ca.gov/ihss/ • Department of Health Care Services – information on refugees • http://www.dhcs.ca.gov/Pages/default.aspx • Juvenile Justice • Law Enforcement • Alcohol and Drug Programs: • http://www.adp.cahwnet.gov/
Acknowledgements DMH/MHSOAC Emily Nahat Jennifer Clancy Nichole Davis Rachel Guerrero Barbara Marquez Sonia Mays Sheri Whitt Beverly Whitcomb Lois Williams CMHDA Alfredo Aguirre Bill Arroyo Nancy Peña Dan Souza Stephanie Welch UCD CRHD Sergio Aguilar-Gaxiola Joshua Breslau Leticia Carrillo Natalia Debb-Sossa Katherine Elliott Ron King Cristina Magaña Arnulfo Medina Elizabeth Miller Marbella Sala Bill Sribney