Download
1 / 71
740 likes | 1.56k Views
Spinal Cord Injuries. Prepared by: Mrs Raheegehn Awni 16/03/2012. INTRODUCTION. Acute spinal cord injury primarily affects young, otherwise healthy males ( 18 to 35 years) A male to female ratio of 3 to 1. 10-15 per million population in UK

E N D
Spinal Cord Injuries Prepared by: Mrs Raheegehn Awni 16/03/2012
INTRODUCTION • Acute spinal cord injury primarily affects young, otherwise healthy males ( 18 to 35 years) • A male to female ratio of 3 to 1. • 10-15 per million population in UK The permanent paralysis experienced by these 800 or so patients a year leads to • major disability, • a shorter life expectancy • significant economic costs.
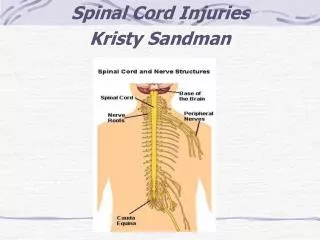
Definition • Spinal cord injury (SCI) is damage to the spinal cord that results in a loss of function such as mobility or feeling. • In most SCI cases, the spinal cord is intact, but the damage to it results in loss of function.
( SCI ) • Associated with car accidents, sports injuries, and other violent impacts. • The degree of paralysis is directly related to the level and severity of the injury. • Injury below the first thoracic vertebra may produce paraplegia. • Injuries above the first thoracic vertebra may cause quadriplegia.
Advances in the management of spinal cord-injured patients have resulted in an improvement in overall survival and quality of life. • The stability of the spine is dependent on the integrity of the anterior, middle and posterior columns.
Causes and Symptoms • According to the National Spinal Cord Injury Association (NSCIA), spinal cord injuries are caused in the United States by motor vehicle accidents (44%), • acts of violence (24%), • falls (22%), sports (8%), • and other causes (2%) such as abscesses, tumors, polio, spina bifida
SCI symptoms • usually appear immediately after the injury. • However, symptoms can develop slowly, if an infection or tumor is gradually increasing pressure on the spinal cord. • weakness, poor coordination or paralysis, particularly below the level of the injury • numbness, tingling, or loss of sensation • loss of bowel or bladder control • pain
NEUROGENIC SHOCK • In acute spinal cord injury, shock may be neurogenic, haemorrhagic, or both. • Following injuries at or above T6 there is significant loss of the sympathetic autonomic outflow. • Consequently vasomotor tone is reduced and, if the lesion is high enough, sympathetic innervation of the heart ceases. • This loss of sympathetic tone results in hypotension and also enhances vagal reflexes, causing profound bradycardia.
Spinal shock • Spinal shock is defined as the complete loss of all neurological function, including reflexes, rectal tone and autonomic control below the level of spinal cord injury. • Spinal shock is unrelated to hypovolaemia or neurogenic shock involves a 24- to 72-h period of complete loss of sensory, motor and segmental reflex activity with flaccid paralysis and areflexia below the level of the injury. • Despite this profound paralysis, areas of the cord are still capable of a full recovery.
Diagnosis • The possibility of SCI is usually suspected in anyone with significant trauma to the head and/or neck. • Assume that such patients have a spine fracture until proven otherwise. • x-rays of the spine • CT scan (computed tomography), MRI (magnetic resonance imaging), and myelogram (x ray after injection of dye into the spinal canal).
ASSESSMENT AND MANAGEMENT OF PATIENTS WITH SPINAL INJURY • Reasons for missing significant spinal injuries are failing to consider injuries in patients who are either unconscious, intoxicated or have pre-existing risk factors (such as arthritis), • Failing to examine patients adequately, and errors in the interpretation of radiographs • Failing to examine patients adequately
AIRWAY WITH CERVICAL SPINE CONTROL AND BREATHING • During assessment of Airway, Breathing and Circulation, efforts must be made to protect the spinal cord from potential secondary injury. This is assisted by early immobilization of the whole spine.
SPINAL IMMOBILIZATION • The majority of trauma patients will have been immobilized during the pre-hospital phase. • The adequacy of immobilization and the position of and cervical collars. • If none is in place, immobilization can be achieved by holding the head in the neutral position, or by the use of head blocks and tape.
Patients who are agitated and moving around should not have their cervical spine immobilized in isolation. • Long spine boards should be removed as soon as possible in a controlled way, usually as part of the log-roll. • This will decrease the risk of pressure sore development in the spinally injured. • Do not leave patients on long spine boards: remove them during the log-roll
The airway is the first priority • A jaw thrust, clearing of oral secretions and insertion of oral or nasal airway may be all that is required initially to maintain the airway. • Supplemental oxygen should be administered to prevent secondary damage from hypoxia. • The whole spine must be maintained in neutral alignment after gentle controlled movement to a neutral position • Attempts to bring the head into neutral alignment against palpable resistance or if the patient complains of pain should be abandoned and the head immobilized as it is found.
Unconscious trauma patients should have orotracheal intubation. • In conscious patients with signs of a high spinal cord injury (for example, weakness in arms and legs, neurogenic shock or diaphragmatic breathing) early intubation and ventilation should be considered. • Intubation is not contraindicated in the presence of spinal injury.
The ideal technique is intubation with cervical spine control. • Oral suction, laryngoscopy and intubation may precipitate severe bradycardia from unopposed vagal stimulation in patients with autonomic disruption from cervical or high thoracic spinal cord injury. • Atropine should be immediately available.
CIRCULATION The most common sources of occult haemorrhage are: • chest injuries (often associated with thoracic spine fractures) • intra-abdominal haemorrhage • retroperitoneal haemorrhage • pelvic fractures and long-bone fractures.
Once occult sources of haemorrhage have been excluded, initial treatment of neurogenic shock involves cautious fluid resuscitation. • Excessive fluid administration may precipitate pulmonary oedema. • The therapeutic goals for neurogenic shock are adequate perfusion with a systolic blood pressure of 90-100 mmHg), a heart rate of 60-100 beats per minute, urine output above 30 ml/h, and normothermia. • Patients with persisting bradycardia should be given atropine 0.5-1 mg intravenously, this being repeated if necessary until the heart rate is acceptable.
THE LOG-ROLL • A log-roll should be performed at the end of the primary survey. • This allows assessment of the back and spinal column and the removal of the long spine board if one is present. • Before the log-roll is commenced, mechanical stabilization of the cervical spine should be removed and replaced by manual in-line immobilization by the log-roll team leader.
At the same time, the neck can be checked for any deformity, tenderness, bogginess or spasm. • To examine the remainder of the vertebral column the patient must be 'log-rolled'.
This technique requires at least five people. • One person is responsible for maintaining the in-line stabilization of the head and neck and coordination of the log-roll (the team leader). • A second person holds the patient's shoulder with one hand and places the other hand on the pelvis.
The third person holds the pelvis with one hand and places the other hand under the patient's opposite thigh. • The fourth person places both arms under the opposite lower leg and supports it during the roll.
The fifth person is responsible for examining the back, conducting a rectal and perineal examination, observing pressure areas, and clearing debris.
Further staff will be needed to assist with the removal of a long spine board. • The team leader must give clear audible instructions and indicate in advance what these will be: • 'The instruction will be ready, steady, move'.
The examination of the back • includes looking for evidence of bruising or swelling, palpation over the spinous processes for deformity, swelling, wounds or increased tenderness down the whole length of the spine. Local tenderness at any point should be used to guide radiographic examination.
Patients with altered level of consciousness or other distracting injuries may not have any features on examination of the back to suggest spinal injury, and may be unable to cooperate with neurological examination. • Despite these, spinal injury cannot be absolutely excluded until a full neurological and radiological examination has been completed.
These patients will require spinal immobilization until they regain consciousness.
Signs of spinal injury in the unconscious patient • Diaphragmatic breathing • Neurogenic shock (hypotension and bradycardia) • Flaccid areflexia (spinal shock) • Flexed posture of the upper limbs (loss of extensor innervation distal to C5) • Response to pain above the clavicles only • Priapism (the erection may be incomplete)
Trauma in women • Trauma in women includes accidental injury to the pregnant woman and to the fotus, and to the gynaecological organs in association with major trauma to the abdomen and pelvis. • Also included is deliberate injury, encompassing domestic violence.
When managing trauma in any female patient aged between 10 and 60 years, the • possibility of pregnancy must be considered. • Not one, but two lives may be at risk and initial assessment and ongoing monitoring must include the fetus.
Outcome for the fetus is dependent upon successful management of the mother. • A multidisciplinary approach is demanded, with early involvement of an obstetrician • A neonatal paediatrician if appropriate, in addition to the usual members of the trauma response team
In most cases these injuries are slight and are the result of falls or direct blows to the abdomen. Complications associated with pregnancy occur in over 8% of women admitted to hospital. The risk of foetomaternal transfusion must be considered in all cases beyond 11 weeks'
complications • slight injury: • premature labor, • Placental abruption • injury to the fetus. • In a minority of cases, life-threatening maternal and fetal injury will occur. • For example, trauma remains the most common cause of non-obstetric death.
MECHANISMS OF INJURY These include: • Road traffic accidents • Motorcycle and bicycle accidents • Burn injury • Intentional injury • Falls • Exposure to blast
Blunt impact • Road traffic accidents (RTAs) still predominate among blunt impact trauma cases, and deaths from head and intra-abdominal injury are the leading cause of non-obstetric mortality. • Invariably this also results in fetal death; maternal death remains the most common cause of fetal death, followed by placental abruption.
Domestic violence • Is typically characterized by direct blows to the abdomen. • Falls are another common cause of maternal and fetal injury. • Seat belts have been shown to reduce maternal mortality, though poorly applied or designed restraints may increase fetal mortality
belt placed above the pregnant uterus reduce the risk of injury to the fetus, particularly due to placental abruption. • The abdominal wall musculature, the pregnant uterus and amniotic fluid all afford some protection to both mother and fetus by absorbing applied forces.
However, acceleration, deceleration and shearing forces or direct blows applied to the abdominal wall in later pregnancy may result in placental abruption, with or without disseminated intravascular coagulation, ruptured uterus and direct injury to the fetus.
Farmer et a/.12 have shown that the extent of maternal injury does not necessarily correlate with the degree of fetal injury. • Lethal fetal injury associated with placental disruption or direct injury may occur in the face or minimal maternal injury.
Penetrating injury • penetration by vehicular parts or debris from the environment (fences or railings); • stab injury by knives or related objects; • In the UK, the usual pattern of injury is by stabbing or penetration by objects in RTAs, or following falls.
During the first trimester, patterns of injury in thepregnant and non-pregnant woman are similar, provided that the injury track does not extend into the pelvis. • In later pregnancy the uterus acts a shield for the mother, but the fetus is at particular hazard.
The uterine musculature and the amniotic fluid effectively retard missile velocity, reducing energy transfer and wounding potential, with outcome for the fetus being determined by the structures injured. • Penetration of the umbilical cord or placenta may result in abruption and haemorrhage, which may be catastrophic for both fetus and mother.
Operative intervention is recommended in all cases of penetrating injury in the • pregnant woman. • At laparotomy, the uterus must be carefully assessed for evidence of penetration and the viability of the fetus assessed.
Evidence of uterine penetration is widely regarded as an indication for immediate Caesarean section. In early pregnancy (less than 28 weeks), operative delivery of the fetus is associated with risk of fetal death, and it may be appropriate in carefully selected cases to preserve the pregnancy.