Download
1 / 26
270 likes | 442 Views
Screening ART Patients for Cardiovascular Disease Risk Factors. The Medtronic Study March 26, 2014. The Medtronic Study. Description of the study Operational challenges. Study Background. The intersection of HIV and NCDs has been of interest to ICAP for several years

E N D
Screening ART Patients for Cardiovascular Disease Risk Factors The Medtronic Study March 26, 2014
The Medtronic Study • Description of the study • Operational challenges
Study Background • The intersection of HIV and NCDs has been of interest to ICAP for several years • Can the systems, tools and approaches used for HIV be leveraged to support NCD services for the general population? • Can we/should we integrate screening for NCDs into HIV programs? • We have conducted two small studies, one in Swaziland and one in Ethiopia • We received funding from Medtronic Philanthropy to conduct a small pilot study in SA
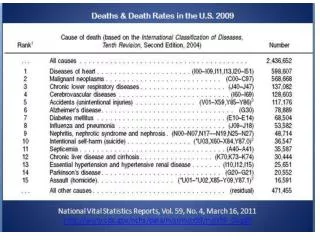
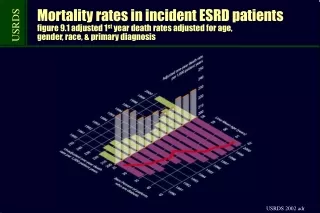
Study Background • Although HIV remains a leading cause of death amongst adults in South Africa, the burden of cardiovascular disease is high and rising • CVD is responsible for 11% of total deaths in SA • The successful scale-up of HIV care and treatment means that people living with HIV (PLWH) are living longer and at risk for other illnesses • PLWH are at higher risk of CVD than their peers
Study Background • The best way to integrate HIV services and the management of CVD risk factors is unknown • Can we provide effective services in the context of HIV care? • Developing strategies that effectively reduce CVD risk, optimize the use of resources, and do not undermine HIV-related program and patient outcomes is an important challenge • Aligned with NDOH priorities and policies
Study Background Two approaches of interest are: • The use of streamlined screening models, including point-of-care diagnostics • Algorithm-guided management using risk prediction charts The Medtronic study explores both of these approaches
Study Design • Pilot study • Cross-sectional design • Single site (the Zamdela CHC in Free State) • 300 patients • Single visit • Vital signs, chart abstraction, questionnaire, POC and lab tests • Assess presence/absence of CVD risk factors • Determine 10 year risk of CVD event • Provide appropriate counseling and referrals
Study Outcomes Primary outcomes: • Prevalence of selected CVD risk factors amongst adults on ART Secondary outcomes: • Percentage of participants at > 20% ten year risk of a cardiovascular event • Comparison of POC and laboratory results • Association of sociodemographic and HIV disease characteristics with key evaluation outcomes
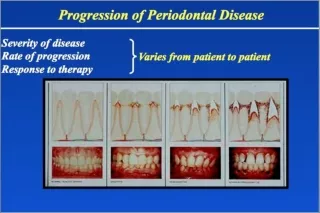
CVD Risk Stratification • Uses multiple variables to estimate the 10-year risk of a major cardiovascular event (heart attack, stroke) • Treatment decisions guided by 10-year risk, not presence/absence of individual risk factors • BP of 160/85 is approached differently for a 40 year-old woman with no other risk factors vs. a 60 year-old male smoker with elevated cholesterol and diabetes
Risk Indices • There are several validated CVD risk indices • The Framingham index is the most famous • WHO and the International Society of Hypertension developed a risk index for low- and middle-income countries • Based on available epidemiologic data for specific sub-regions • Reflects likely access to diagnostic testing (or lack thereof)
Example • 40 year-old woman • Non-smoking • No diabetes • SBP 160 • Total cholesterol of = 6 mmol/L
Why are we using risk stratification in the HEART study? • We want to pilot an approach that is realistic to use in busy HIV clinics in resource limited settings • Risk stratification enables programs to prioritize resources and referrals
How are we using risk stratification in the HEART study? • Study nurses will collect key data @ study visit • Sex, age (from participant questionnaire) • Smoking status (from participant questionnaire) • Systolic BP (with vital signs) • HbA1c (POC test) • Total cholesterol (POC test) • These will be used to determine preliminary risk stratification for participants > 40 years
How are we using risk stratification in the HEART study? • In order to explore the potential of this approach, we have decided to use both POC testing and laboratory testing • Preliminary risk stratification will use POC results • Final risk stratification will use laboratory results • One of our outcomes is the number of participants whose risk stratification changed once lab results were available
How are we using risk stratification in the HEART study? Preliminary risk stratification will be used to guide follow up for participants > 40 years: • All participants will receive post-test counseling • Those with < 10% risk will follow up with their HIV clinic nurse as per routine • Those with 10-30% risk will follow up with their HIV clinic nurse within 4 weeks • Those with > 30% risk will have a same-day appointment with the NCD doctor or a professional nurse at Zamdela CHC
How are we using risk stratification in the HEART study? • Final risk stratification will be performed once the laboratory results are available, generally within 2 days. • If the results of final risk stratification change recommended management, the participant will be called with the information and a new appointment
CVD Risk Management Algorithm *In both categories, participants with newly identified diabetes and/or hypertension should be screened for red flag symptoms. If present, they should be provided with risk-factor specific counseling and referred for same-day appointment with NCD doctor / OPD clinic. *In the unlikely event that the NCD doctor is unavailable, participants will be referred to the Professional Nurse(s) in charge at Zamdela Community Health Centre.
What will we learn? • The distribution of CVD risk amongst a subset of the ART clinic population • To what extent the preliminary risk stratification differs from the final risk stratification • i.e., the utility of laboratory testing vs. POC testing • To what extent participants complete their referrals
What will we do with the results? • If the prevalence of CVD risk is very low, policy-makers may conclude that routine screening is not a priority • If the prevalence is not very low, we are interested in testing the integration of risk-stratification into the HIV clinic • If the use of rapid screening and risk stratification with POC testing seems feasible, this is the model we would like to test in future
Operational Challenges Where are we now?
Challenge #1: Research Partners • Given the study budget and limited availability of ICAP-SA staff, we decided to hire a local research partner to conduct data collection • Selected ACRO (the African Clinical Research Organization) in September 2013 • Initial plan was for: • Local service agreement for start-up activities • ICAP-NY subaward for study implementation
Challenge #1: Research Partners • Local service agreement executed w/o difficulty • ICAP-NY suggests service agreement rather than subaward • Review of service agreement package at CU unexpectedly complex • ex: Risk Management requires ACRO to have indemnity insurance to cover potential “bodily injury” (e.g. from phlebotomy) • ex: Legal asks: Who will insure the vehicles in which the study nurses drive to work?
Challenge #2: Timeframe • Start up delayed by two months • Initial recruitment considerably slower than planned • Grant ends in May 2013 • Will need to ask for no-cost extension (already informally approved by Medtronic)
Next Steps • No-cost extension • Data collection • Data analysis…