Download
1 / 28
320 likes | 584 Views
RENAL SYMPATHETIC DENERVATION. Anxiolytic for nervous kidneys???. HYPERTENSION. Is according to the WHO the most frequent cause of death worldwide. In 2025, 50% of the adult population will be hypertensive.

E N D
RENAL SYMPATHETIC DENERVATION Anxiolytic for nervous kidneys???
HYPERTENSION • Is according to the WHO the most frequent cause of death worldwide. • In 2025, 50% of the adult population will be hypertensive. • 20-30% of patients are considered to have resistant HTN despite availability of potent medications.
HYPERTENSION • 20/10mmHg increase in blood pressure doubles cardiovascular mortality. • Reduction of systolic blood pressure by only 10 mmHg reduces the risk of stroke by 30%. • 7.5 million deaths annually.
HYPERTENSION • Only half of all treated hypertensives are controlled to established BP targets. • High prevalence: • Affects 1 in 3 adults. • 1B people worldwide 1.6 B by 2025 35% Treated but Uncontrolled 30% Untreated 35%Treated &Controlled Chobanian et al. Hypertension. 2003;42(6):1206–1252. 5
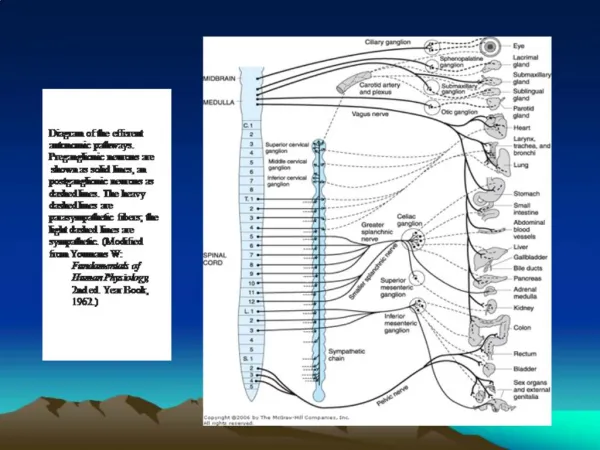
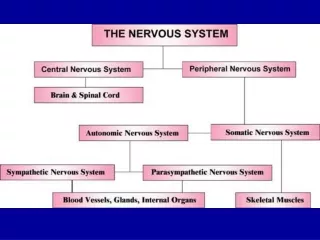
Renal Sympathetic Activation: Efferent NervesKidney as Recipient of Sympathetic Signals Renal Efferent Nerves ↑ Renin Release RAAS activation ↑ Sodium Retention ↓ Renal Blood Flow 6
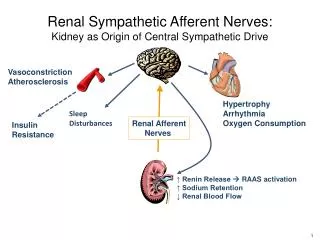
Renal Sympathetic Activation: Afferent NervesKidney as Origin of Central Sympathetic Drive Vasoconstriction Atherosclerosis Hypertrophy Arrhythmia Oxygen Consumption Sleep Disturbances Renal Afferent Nerves Insulin Resistance ↑ Renin Release RAAS activation ↑ Sodium Retention ↓ Renal Blood Flow 7
Initial Cohort – Reported in the Lancet, 2009: • First-in-man, non-randomized • Cohort of 45 patients with resistant HTN (SBP ≥160 mmHg on ≥3 anti-HTN drugs, including a diuretic; eGFR≥ 45 mL/min) • 12-month data
Renal Nerve Anatomy • Nerves arise from T10-L2 • Follow the renal artery to the kidney • Primarily lie within the adventitia. Vessel Lumen Media Adventitia Renal Nerves 11 11
Catheter-Based Approach Spacing of e.g. 5 mm. • Renal artery access via standard interventional technique • Radiofrequency electrode tip • 4-6 two-minute treatments per artery • RF generator • Automated • Low power-max 8 Watts • Built-in safety mechanisms 12
Hypertension. 2011;57:911-917. • Expanded Cohort – This Report (Symplicity HTN-1): • Expanded cohort of patients (n=153) • 36-month follow-up • 90% response rate, >20/10mmHg reduction. 13
The simplicity HTN-2 Trial • Purpose: To demonstrate the effectiveness of catheter-based renal denervation for reducing blood pressure in patients with uncontrolled hypertension. • Study design: Randomized, controlled clinical trial. • Patients:106 patients randomized 1:1 to treatment with renal denervation vs. control. • Participating centres:24 centers in Europe, Australia, & New Zealand.
The simplicity HTN-2 Trial Inclusion Criteria: • -Office SBP ≥ 160 mmHg (≥ 150 mmHg with type II diabetes mellitus) • -3+ more anti-HTN medications • -Age 18-85 years Exclusion Criteria: • -Significant renal artery abnormalities or prior renal artery intervention • -eGFR < 45 mL/min/1.73m2 (MDRD formula) • -Type 1 diabetes • -Contraindication to MRI • -Significant stenoticvalvular heart disease • -MI, unstable angina, or CVA in the preceding 6 months
The simplicity HTN-2 Trial Before randomisation and to assess eligibility: • Screening process required patients to record daily bd automated BP measurements and to document drug compliance for 2/52. • Renal artery anatomical screening, with renal duplex, CT, MRI or renal angiography to confirm anatomical eligibility. • Baseline creatinine, Cystatin C, ACR. • 24hr BP measurement.
Follow up • At 1, 3 and 6 months, with rpt creat, Cystatin C, BP, ACR. • Office and home BP readings, average of 3. • Daily home BP and drug compliance diary 2/52 prior to the 6 month FU. • At 6 months: 24hr BP monitor and renal imaging in the renal denervation group.
. 84% of RDN patients had ≥10 mmHg reduction in SBP. 10% of RDN patients had no reduction in SBP. p <0.001 for difference between RDN and Control
Adverse events • No significant change in renal function. • One renal artery dissection from injection of contrast into renal arter wall during dye angiography. The lesion was stented without further consequences. Minor adverse events (n=52) •1 femoral artery pseudoaneurysm manual compression •1 post-procedural drop in BP resulting in a reduction in medication •1 urinary tract infection •1 prolonged hospitalization for evaluation of paraesthesias •1 back pain treated with pain medications & resolved after one month 6-month renal imaging (n=43) •No vascular abnormality at any RF treatment site •1 MRA indicates possible progression of a pre-existing stenosis unrelated to RF treatment (no further therapy)
Conclusions • Catheter-based renal denervation, done in a multicentre, randomised trial in patients with treatment-resistant essential hypertension, resulted in significant reductions in BP. • The technique was applied without major complications. • This therapeutic innovation, based on the described neural pathophysiology of essential hypertension, affirms the crucial relevance of renal nerves in the maintenance of BP in patients with hypertension. • Catheter-based renal denervation may be beneficial for patients with treatment-resistant essential hypertension.
Limitations • Non-blinded trial. • ?long-term benefit, ?evidence of reinnervation • Small number of patients. • Was the population truly treatment resistant? • Adjustments in medications, unclear effect on pill burden • Effect in patients with more severe CKD. Simplicity HTN-3 trial on way