Download
1 / 18
220 likes | 493 Views
Drug Coated Balloons From Bench to Bedside. Service de Radiodiagnostic et Radiologie Interventionnelle Université de Lausanne. Salah D. Qanadli , MD, PhD, FCIRSE Cardio-Thoracic and Vascular Unit, QMI Lab Department of Radiology CHUV-University of Lausanne. Potential Conflict of Interest.

E N D
Drug Coated BalloonsFrom Bench to Bedside Service de Radiodiagnostic et Radiologie Interventionnelle Université de Lausanne Salah D. Qanadli, MD, PhD, FCIRSE Cardio-Thoracic and Vascular Unit, QMI Lab Department of Radiology CHUV-University of Lausanne
Potential Conflict of Interest • Educational grants • Cordis, Boston Scientific, Medtronic, Invatec, Bard • Research grants • Abbott Vascular, Biotronik, Cordis, St Jude Medical • Consultancy • Mediar Ltd. • University of Kingston London • Cook, Optimed, Cordis, Bard, Abbott, Terumo • Bioclinica
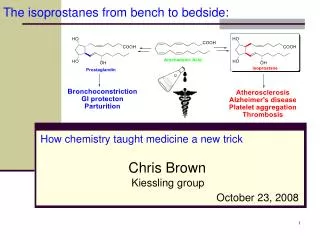
Dotter’s Predictions in World’s First PTA* • Balloon angioplasty • Recanalization devices • Outpatient PTA • Cost saving relative to surgery • Endovascular “splints” (stents) that “reintimalize” (endothelialize) Dotter et al., Circulation, 1964
PTA in 2013 for PAD • Critical issues • Immediate technical results • - Immediate out-come • Flow limiting dissection • Elastic Recoil • Immediate technical success • CTO recanalization • Re-stenosis (mid and long-term patency) DCB Technology
DCB Mechanism of Action • 30-second minimum inflation transfers drug to endoluminal surface • PTX diffuses into the arterial wall from an endoluminal reservoir • Over time, therapeutic drug levels are sustained in deep cell layers after endothelial drug levels become sub-therapeutic • Drug continues to inhibit restenosis in arterial wall while allowing the lumen to restore and re-endothelialize
Coating uniformity • European Product, Data on file. • 6x60 mm Lutonix Drug Coated Balloon – N=5 • 6x60 mm In.Pact Admiral-Paclitaxel-eluting PTA balloon catheter – N=5
Defining Indications for DCB • Clinical needs • Device availability • Proof of concept • Clinical evaluation • Strategy for use/Cost-effectiveness
Defining Indications for DCB • Clinical needs • Clinically driven concept • High risk of re-stenosis • Femoro-popliteal lesions • up to 60 % at 12 mo* • Small vessels BTK • up to 69%** • AV Dialysis access • Re-stenosis/occlusion up 62 % at 12 mo*** *Muradin GS et al., Radiology, 2001. **Krokidis M et al., CardiovascInterventRadiol, 2012. ***Bittl JA, JACC Cardiovascular Interv, 2010.
Defining Indications for DCB • Clinical needs • Clinically driven concept • Limitations of existing alternatives (Stents, including DES) • BTK ? • BTA • AV shunts • FP • ISR • Complex anatomy (bifurcations, trans-collateral approaches,…) • Over dependence of double anti-agregants
Defining Indications for DCB • Technology safety/efficacy • Proof of concept • Paclitaxel coated balloon (PCB) • DCB in routine practice in 2013 is PCB ! • Clinical evaluation • Level of Evidence • Cost-effectiveness • Strategy for use
De-Novo Femoro-popliteal Lesions THUNDER FemPac LEVANT I PACIFIER Control arm: UB ! Median FU: 10.3 mo Exclusion: Severely impaired arterial out flow
Who is the best candidate for PCB ? BTK/BTA ISR AV Dialysis Access
What doses the future hold ? BTK/BTA ISR AV Dialysis Access
“Good judgment is based on experience and experience is based on bad judgment” Martin J. Lipton