Download
1 / 1
10 likes | 113 Views
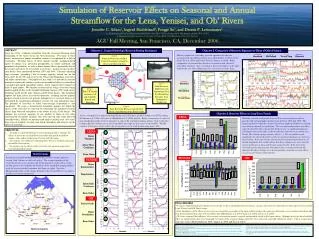
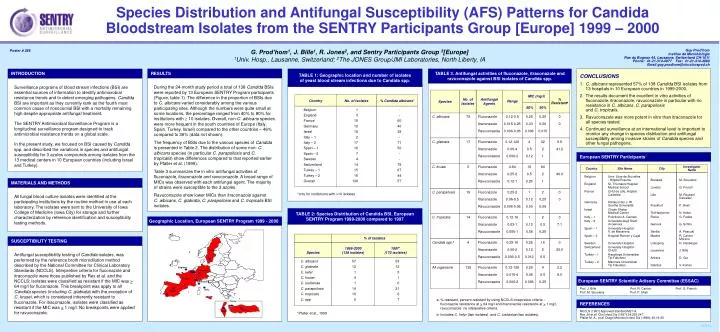
Species Distribution and Antifungal Susceptibility (AFS) Patterns for Candida Bloodstream Isolates from the SENTRY Participants Group [Europe] 1999 – 2000. TABLE 2: Species Distribution of Candida BSI, European SENTRY Program 1999-2000 compared to 1997. Species. % of Isolates. Species.

E N D
Species Distribution and Antifungal Susceptibility (AFS) Patterns for Candida Bloodstream Isolates from the SENTRY Participants Group [Europe] 1999 – 2000 TABLE 2: Species Distribution of Candida BSI, European SENTRY Program 1999-2000 compared to 1997 Species % of Isolates Species 1999-2000(138 isolates) 1997*(170 isolates) Sweden C. albicans C. albicans 57 53 C. glabrata 12 12 C. kefyr 1 0 C. krusei 4 1 C. lusitaniae 1 0 C. parapsilosis 14 21 C. tropicalis 10 6 C. spp 0 7 England Germany C. glabrata Belgiu m France Switzerland Italy Spain C. krusei *Pfaller et al., 1999 Turkey Israel C. parapsilosis TABLE 1: Geographic location and number of isolates of yeast blood stream infections due to Candida spp. C. tropicalis Country No. of Isolates % Candida albicans* Belgium 1 - England 3 - France 15 60 Germany 10 40 Israel 18 39 Italy – 1 2 - Italy – 2 17 71 Spain – 1 16 50 Spain – 2 7 - Sweden 4 - Switzerland 14 79 Turkey – 1 15 67 Turkey – 2 16 44 Overall 138 57 Candida spp.b All organisms *only for institutions with >10 isolates G. Prod’hom1, J. Bille1, R. Jones2, and Sentry Participants Group 3[Europe] 1Univ. Hosp., Lausanne, Switzerland; 2The JONES Group/JMI Laboratories, North Liberty, IA Poster # 266 Guy Prod’hom Institue de Microbiologie Rue du Bugnon 44, Lausanne, Switzerland CH-1011 Phone: 41-21-314-4077 Fax: 41-21-314-4060 Email:guy.prodhom@chuv.hospvd.ch RESULTS TABLE 3. Antifungal activities of fluconazole, itraconazole and ravuconazole against BSI isolates of Candida spp. CONCLUSIONS 1.C. albicans represented 57% of 138 Candida BSI isolates from 13 hospitals in 10 European countries in 1999-2000. 2. The results document the excellent in vitro activities of fluconazole, itraconazole, ravuconazole in particular with no resistance in C. albicans, C. parapsilosisand C. tropicalis. 3. Ravuconazole was more potent in vitro than itraconazole for all species tested. 4. Continued surveillance at an international level is important to monitor any change in species distribution and antifungal susceptibilty among invasive strains of Candida species and other fungal pathogens. INTRODUCTION During the 24-month study period a total of 138 Candida BSIs were reported by 13 European SENTRY Program participants (Figure, table 1). The difference in the proportion of BSIs due to C. albicans varied considerably among the various participating sites. Although the numbers were quite small at some locations, the percentage ranged from 40% to 80% for institutions with ³ 10 isolates. Overall, non-C. albicans species were more frequent in the south countries of Europe (Italy, Spain, Turkey, Israel) compared to the other countries – 46% compared to 36% (data not shown). The frequency of BSIs due to the various species of Candida is presented in Table 2. The distribution of some non- C. albicans species (in particular C. parapsilosis and C. tropicalis) show differences compared to that reported earlier by Pfaller et al. (1999). Table 3 summarizes the in vitro antifungal activities of fluconazole, itraconazole and ravuconazole. A broad range of MICs was observed with each antifungal agent. The majority of strains were susceptible to the 3 azoles. Ravuconazole show lower MICs than itraconazole against C. albicans, C. glabrata, C. parapsilosis and C. tropicalis BSI isolates. Surveillance programs of blood stream infections (BSI) are essential sources of information to identify antimicrobial resistance trends and to detect emerging pathogens. Candida BSI are important as they currently rank as the fourth most common cause of nosocomial BSI with a mortality remaining high despite appropriate antifungal treatment. The SENTRY Antimicrobial Surveillance Program is a longitudinal surveillance program designed to track antimicrobial resistance trends on a global scale. In the present study, we focused on BSI caused by Candida spp. and described the variations in species and antifungal susceptibility for 3 azoles compounds among isolates from the 13 medical centers in 10 European countries (including Israel and Turkey). No. of Isolates AntifungalAgents Range % Resistanta MIC (mg/l) 50% 90% 79 Fluconazole Itraconazole Ravuconazole 0.12-0.5 0.015-0.25 0.006-0.06 0.25 0.03 0.006 0.25 0.06 0.015 0 0 17 Fluconazole Itraconazole Ravuconazole 0.12-128 0.06-4 0.006-2 4 0.5 0.12 32 2 1 5.9 41.2 European SENTRY Participants3 5 Fluconazole Itraconazole Ravuconazole 4-64 0.25-2 0.12-1 16 0.5 0.25 64 2 1 40.0 Country Site Name City InvestigatorName Belgium Univ. Libre de Bruxelles - Hôpital Erasme Brussels M. Struelens England St. Thomas's Hospital Medical School London G. French France CHU de Lille, Hôpital Calmette Lille M. Roussel Delvallez Germany Klinikum der J. W. Goethe Universität Frankfurt P. Shah Israel Chaim Sheba Medical Center Tel-Hashomer N. Keller Italy – 1 Policlinico A. Gemelli Roma G. Fadda Italy – 2 Universita degli Studi di Genova Genova G. Schito Spain – 1 University Hospital V. de Macarena Sevilla A. Pascual Spain – 2 Hospital Ramon y Cajal Madrid R. Canton Moreno Sweden University Hospital Linkoping H. Hanberger Switzerland University Hospital - CHUV Lausanne J. Bille Turkey – 1 Hacettepe Universitesi Tip Fakultesi Ankara D. Gur Turkey – 2 Marmara Universitesi Tip Fakultesi Istanbul V. Korten MATERIALS AND METHODS All fungal blood culture isolates were identified at the participating institutions by the routine method in use at each laboratory. The isolates were sent to the University of Iowa College of Medicine (Iowa City) for storage and further characterization by reference identification and susceptibility testing methods. 19 Fluconazole Itraconazole Ravuconazole 0.25-2 0.06-0.5 0.006-0.06 1 0.12 0.03 2 0.25 0.06 0 0 14 Fluconazole Itraconazole Ravuconazole 0.12-16 0.03-1 0.006-1 1 0.12 0.06 2 0.5 0.25 0 7.1 Geographic Location, European SENTRY Program 1999 - 2000 SUSCEPTIBILITY TESTING 4 Fluconazole Itraconazole Ravuconazole 0.25-16 0.06-2 0.006-0.5 0.25 0.12 0.012 16 2 0.5 0 25.0 Antifungal susceptibilitly testing of Candida isolates, was performed by the reference broth microdilution method described by the National Committee for Clinical Laboratory Standards (NCCLS). Interpretive criteria for fluconazole and itraconazole were those published by Rex et al. and the NCCLS: isolates were classified as resistant if the MIC was > 64 mg/l for fluconazole. This breakpoint was apply to all Candida species (including C. glabrata) with the exception of C. krusei, which is considered inherently resistant to fluconazole. For itraconazole, isolates were classified as resistant if the MIC was > 1 mg/l. No breakpoints were applied for ravuconazole. 138 Fluconazole Itraconazole Ravuconazole 0.12-128 0.015-4 0.006-2 0.25 0.06 0.006 4 0.5 0.25 2.2 8.0 European SENTRY Scientific Adisory Committee (ESSAC) Prof. J. Bille Prof. R. Canton Prof. G. French Prof. M. Struelens Prof. P. Shah a: % resistant, percent resistant by using NCCLS interpretive criteria : fluconazole resistance at > 64 mg/l and itraconazole resistance at > 1 mg/l, ravuconazole: no interpretive criteria. b: Includes C. kefyr (two isolates) and C. lusitaniae (two isolates). REFERENCES NCCLS (1997) Approved standard M27-A. Rex JH et al. Clin Infect Dis (1997) 24:235-247. Pfaller M. A., et al. Diagn Microbiol Infect Dis (1999); 35:19-25. A156-21