Download
1 / 23
340 likes | 2.23k Views
PLACENTA PRAEVIA. Associate Professor Iolanda Elena Blidaru Md, PhD. PLACENTA PRAEVIA. Definition P lacenta praevia = placental insertion over or very near the internal os of the cervix (in the lower uterine segment including the zone of effacement and dilatation).

E N D
PLACENTA PRAEVIA Associate Professor Iolanda Elena Blidaru Md, PhD.
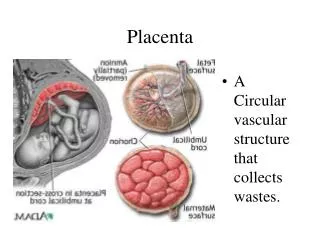
PLACENTA PRAEVIA Definition • Placenta praevia = placental insertion over or very near the internal os of the cervix (in the lower uterine segment including the zone of effacement and dilatation). • obstacle in front of the presenting part • the most frequent cause of third trimester bleeding
PLACENTA PRAEVIA Classification Depending if the placenta covers the internal cervical os completely or partially: • Total placenta praevia • Partial placenta praevia • Marginal placenta praevia • Low-lying placenta (laterally inserted placenta)
PLACENTA PRAEVIA This classification is made on the basis of findings at the initial examination and may change in labor or as pregnancy advances.
PLACENTA PRAEVIA Incidence • 0.5% -1% of all births • US of early pregnancies - a large number of low-lying pregnancies subsequently aborted. • "placental migration" (US evaluation) → as pregnancy advances, the lower uterine segment lengthens and the placenta is drawn upward with the enlarging uterus.
PLACENTA PRAEVIA Risk factors • previous cesarean section (x 6) • multiparity(x 2.6) • advanced age • previous D&C • smoking
PLACENTA PRAEVIA Etiology • inflammatory or atrophic changes of the endometrium (endometritis, hypoplasia, submucousmyomas, trauma)→ defectivedecidualvascularization • twin pregnancy, with large placental bed • increased surface of the placenta implanted in the lower uterine segment (tissues → unappropriate for nidation)
PLACENTA PRAEVIA Pathogenesis • painless bleeding → maternal blood + fetal blood (a little part). Mechanisms: • separation of the placenta from its implantation site • formation of the lower uterine segment • effacement and dilatation of the cervix in labor • rupture of the venous lake in the deciduabasalis
PLACENTA PRAEVIA Associated conditions • placenta accreta → abnormally firm adherence to the uterine wall • placenta increta → placental villi invade the myometrium • placenta percreta → placental villi penetrate through the myometrium
PLACENTA PRAEVIA Clinical findings • painless bleeding (maternal origin) • slight or profuse hemorrhage • the blood is bright red • postpartalexcessive hemorrhage→ • abnormal adherence, • excessively large area of attachement, • the poorly contracted lower uterine segment, • lacerations in the cervix and lower segment.
PLACENTA PRAEVIA Diagnosis • abdominal examination: abnormal fetal presentation (transverse lie, breech presentation), the presenting part is high above the inlet and deviated anteriorly or laterally • FHR - normal • If cervical os dilated → cautious inspection • digital examination is never permitted unless at term pregnancy, in an operating room with all the preparations for immediate cesarean section; the examination can cause life-threatening hemorrhage.
PLACENTA PRAEVIA Diagnosis Sonography • transabdominal US (96% accuracy) • transvaginal US • transperineal US
PLACENTA PRAEVIA Differential diagnosis • Cervical bleeding → benign / malignant lesions • Endouterine bleeding: • premature separation of the normally implanted placenta, • rupture of umbilical cord vessels, • premature labor.
PLACENTA PRAEVIA DELIVERY MODE Practically all women do need cesarean section.
PLACENTA PRAEVIA CONDUCT AT THE DELIVERY Several clinical situations: 1. The patient is in labor → cesareansection 2. The fetus is mature and the bleeding does not stop → cesarean section 3. The fetus is preterm and there is no indication for delivery → observe 4. The bleeding is so severe, despite the fetus immaturity → cesarean section 5. Total placenta praevia with dead fetus →cesareansection (the bleeding cannot be controlled).
PLACENTA PRAEVIA CONDUCT AT THE DELIVERY • If placenta praevia+accreta, other methods of hemostasis: • oversewing the implantation site • bilateral uterine / inernal iliac artery ligation • packing the lower uterine segment with gauze • total abdominal hysterectomy.
PLACENTA PRAEVIA CONDUCT AT THE DELIVERY Vaginal delivery may be possible in: • a multipara with a soft, effaced and partially dilated cervix + a minor degree of anterior placenta praevia + ruptured membranes • if the fetus is dead, the cervix is soft and effaced, only an edge of placenta can be felt and bleeding is minimal • before the 28th week, when the baby has little chance of surviving
PLACENTA PRAEVIA ADDITIONAL TREATMENT • adequate transfusion • prophilactic treatment of thrombo-embolism / infectious complications • anti-D Ig • bed rest
PLACENTA PRAEVIA Prognosis Maternal Fetal / Neonatal The perinatal mortality rate → 15-20% (10 times>) Causes: • prematurity (a major cause) • IUGR • intrauterine anoxia (placental separation, prolapsed cord) • respiratory distress syndrome • exsanguination • fetal malformations