Download
1 / 18
180 likes | 518 Views
一般醫學系臨床病理討論會. Clinical Pathology Conference 討論篇. 報告者:第 年住院醫師. Hospital course. PB smear Anisocytosis: 3+ Microcytosis: 1+ Chromic: normochromic Fragmented RBC: found Hemolytic anemia was confirmed

E N D
一般醫學系臨床病理討論會 Clinical Pathology Conference討論篇 報告者:第 年住院醫師
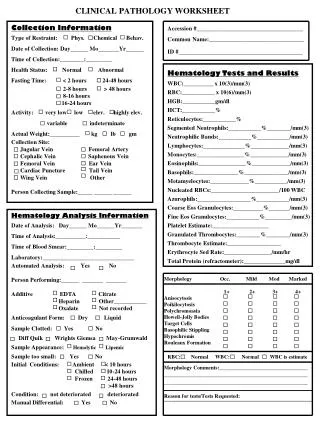
Hospital course • PB smear • Anisocytosis: 3+ • Microcytosis: 1+ • Chromic: normochromic • Fragmented RBC: found • Hemolytic anemia was confirmed • unconjugated hyperbilirubinemia, nucleated red cells, increased RDW, anisocytosis, fragmented RBC
Hospital course • Summary of abnormality • Thrombocytopenia • Conscious disturbance • Hemolytic anemia • Three of the pentad of thrombotic thrombocytopenic purpura (TTP) was matched • No other feasible diagnosis can explain all the abnormality
Hospital course • Plasmaphoresis was arranged • Dexamethasone was given • Empiric antibiotics was prescribed because of fever up to 38.4℃ after admission • Two days after admission, an episode of generalized-tonic-clonic seizure occurred. Diazepam and phenytoin were used. The CT of brain was arranged and there was no intracranial hemorrhage
Hospital course • Her conscious level didn’t improve after all this therapeutic management • Bradycardia then asystole occurred at the second hospital day. Cardiopulmonary resuscitation was performed but failure.
Thrombotic thrombocytopenic purpura (TTP) • Potentially fatal disorder • characterized by platelet aggregates in microvasculature • vessel occlusion • tissue ischemia and end-organ damage • Male: female ratio of 1: 2 • Prompt diagnosis is mandatory • so emergency treatment can be instituted immediately Current Opinion in Neurology. 2003;16:367-73,Hematol Oncol Clin North Am. 2003;17: 177-99, .
Etiology and precipitating factor • Pregnancy • Drugs • e.g. ticlopidine, clopidogrel, oral contraception, cyclosporin, mitomycin C and quinine • Autoimmune disorders • such as SLE • Infection • particularly HIV, toxigenic strains of Shigella and Escherichia coli • Post bone marrow or solid organ transplantation • Post coronary artery bypass graft- 13 cases reported W V Med J.2004; 100(2): 64-6.
Pathophysiology • von Willebrand factor (vWF) • endothelial cells and megakaryocytes normally make monomers of vWF that are joined to form larger vWF multimers • Under normal conditions, vWF-cleaving metalloprotease (ADAMTS13)cleaves these multimers
Clinical and laboratory features • Classical pentad (complete pentad< 30%) • Thrombocytopenia (platelet count < 20×103) • Microangiopathic hemolytic anemia (MAHA) • Neurologic impairment (63-70%) • Renal impairment (59%) • Fever • Chest pain, abdominal pain
Clinical and laboratory features • RBC fragmentation (schistocytes) • ↑ Reticulocyte (increased RBC turnover) • ↓ Haptoglobin (binding to free Hb) • ↑ LDH (hemolysis, ischemic organs) • Renal or liver impairment (representing ischemic organs) • ↑ Unconjugated (indirect) bilirubin • DAT (direct Coombs test) negative • Normal coagulation studies
Treatment • Plasma exchange (mainstay of therapy ) • Superior to plasma infusion • Instituted within 24h of presentation • 1.0-1.5 plasma volume exchanges qd (40 mL/kg) • LDH, usually used as a day-to-day indicator of the severity of hemolysis, along with Hb value and reticulocyte count • In the Canadian Apheresis Trial, complete remission is defined as normalization of platelet count for 2 consecutive days with no deterioration in neurological status
Treatment • Cryosupernatant (cryoprecipitate-poor plasma) • lacking vWF • at least as effective as FFP
Adjunctive therapy • Corticosteroids • methylprednisolone 1g IV qd, or prednisolone 1mg/kg PO qd • Antiplatelet agents • aspirin and dipyridamole • not accepted universally, and might exacerbate the risk of bleeding • RBC transfusion as needed
Contraindications • Platelet transfusions • Desmopressin (DDAVP) • releasing vWF from the endothelial cells into blood
Refractory TTP and Immunosuppressive therapies • Vincristine (Immunosupression) • case reports or small retrospective studies • Rituximab (anti-CD20 Ab) • first use in recent reports • Splenectomy • removal of the B cells responsible for the production of autoantibodies inhibiting ADAMTS13