Download
1 / 17
170 likes | 173 Views
Explore the emergence of new aspects in the longstanding issue of bacterial resistance to antibiotics, including the rise of MRSA, VRSA, and ESBL-producers. Learn about the mechanisms and types of resistance, as well as the epidemiology and major causes of nosocomial infections.

E N D
Bacterial Resistance to Antibiotics: New Facets to an Old Threat By Professor Vincent C. Okore Dean Faculty of Pharmaceutical Sciences University of Nigeria, Nsukka Vincent C. Okore
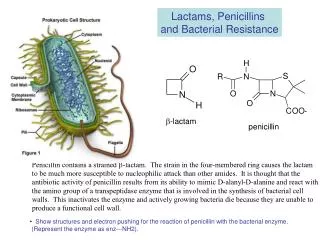
What is Bacterial Resistance? • A clinical situation where the normal therapeutic dose of an antibiotic cannot eliminate an existing infection. • Where an earlier established MIC of an antibiotic cannot inhibit a bacterial species, in vitro. Vincent C. Okore
Epidemiology of Bacterial Resistance: The case of Staphylococcus aureus • S. aureus is a versatile and dangerous pathogen that has been a major cause of morbidity and mortality. • One of the most common causes of nosocomial and community-acquired infections worldwide. • S. aureus infections are often acute and pyogenic. • Have potentials for spreading to surrounding tissues. • Some diseases caused by S. aureus include: bacteremia, pneumonia, osteomyelitis, endocarditis, empyema, toxic shock syndrome, post-operative wound infections, abscesses of the muscle, abscesses of intra-abdominal organs, etc. Vincent C. Okore
Major Cause of Nosocomial Infections • Leading overall cause of nosocomial infections (followed by CoNS). • Widespread use of prosthetic and in-dwelling devices. • Growing number of immuno-compromised patients in hospitals. • Must be managed clinically with effective antibiotics. Vincent C. Okore
Targets of Antibiotic Action Vincent C. Okore
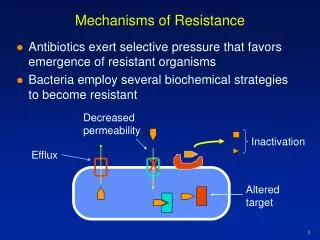
Mechanisms of Resistance • Modification of target enzymes: • DHA synthetase increases its preference to PABA in place of sulphonamides • DHA reductase loses its affinity for trimethroprim or pyrimethamine. • RNA polymerase loses its binding affinity to rifampicin. • DNA gyrase loses its affinity for the fluoroquinolones. • Modification of target sites: • P-10 protein of 30 S subunit of bacterial ribosomes loses its binding power for streptomycin. • The 50 S subunit of bacterial ribosome loses its binding power to streptomycin. • PBP of Streptococcus pneumoniae lose their affinity for benzyl penicillin. Vincent C. Okore
Mechanisms of Resistance contd. • Reduction of physiological importance of target organelles: • G –ve bacteria depend less on peptidoglycan-based cell wall for structural integrity (as compared with G +ve bacteria). • G –ve organisms are resistant to antibiotics that inhibit peptidoglycan synthesis, e.g. penicillins and cephalosporins. • Reduction of uptake of the antibiotic by bacterial cells: • Increased production of protective cell coating that prevents uptake of antibiotics. Occurs through mutation. Vincent C. Okore
Mechanisms of Resistance contd. • Active efflux of antibiotics from the cell • Resistance of various bacterial species to tetracycline. • Resistance of S. aureus to fluoroquinolones. • Production of inactivating enzymes. Resistance is due to production of: • Beta-lactamases that inactivate penicillins, cephalosporins and carbapenems. • Phosphorylases, adenylases and acetylases that inhibit gentamicin and chloramphenicol. Vincent C. Okore
Types of Bacterial Resistance • Innate, e.g. Gonococci against sulphonamides. • Acquired, e.g. Staphylococci against beta-lactams. • Induced, e.g. P. aeruginosa against gentamicin. • Cross, e.g. MRSA & ESBL producers & enterococci against aminoglycosides. • Multiple, e.g. MRSA & CoNS. Vincent C. Okore
THE NEW FACETS: Emergence of MRSA, VRSA & ESBL-Producers The next three slides show statements from different sources indicating clearly that we are encountering new aspects in the old threat of bacterial resistance to antibiotics. Vincent C. Okore
“Occurrence and proliferation of MRSA strains are a cause of major concern not only in the clinical environment but also in community life, since few agents can treat infections by these organisms. In fact, MRSA is resistant to virtually all kinds of β-lactams.” Shibata, H. et al. (2005). Alkyl gallates, intensifiers of β-lactam susceptibility in methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 49:549-555. Vincent C. Okore
“In 1996, a S. aureus strain with intermediate resistance (MIC = 8 µ/ml) to vancomycin was first isolated from a patient in Japan. Shortly afterward, VISA strains were isolated in USA, Europe and some Asian countries. The mechanisms of resistance are complex involving changes in cell wall contents and composition. In 2002, the world’s first reported case of S. aureus with high resistance (MIC > 128 µ/ml) to vancomycin was diagnosed in a patient in the USA.” Chakraborty, S. P. et al. (2011). Isolation and identification of vancomycin resistant Staphylococcus aureus from post operative pus sample. Al Ameen J. Med. Sci. 4: 152-168. Vincent C. Okore
“ESBLs are bacterial enzymes that hydrolyse and confer resistance to modern cephalosporin antibiotics … (e.g. cefuroxime, cefotaxime, ceftriaxone and ceftazidime). An unfortunate discovery is that ESBL-producing organisms often also possess resistance determinants to other important antibiotic groups, such as aminoglycosides and fluoroquinolones, leaving an extremely limited range of effective agents.” Afunwa, et al. (2011). Antimicrobial resistance status and prevalence rates of extenced spectrum beta-lactamase producers isolated from a mixed human population. Bosnian J. Basic Med. Sci. 11: 91-96. Vincent C. Okore
Antibiotic susceptibility profile of 30 strains of Staphylococcus aureus Pen: Penicllin G; Amp: Ampicillin; Cep: Cephotaxime; Gen: Gentamicin; Str: Streptomycin; Tet: Tetracycline; Ery: Erythromycin; Chl: Chloramphenicol; Nx: Norfloxacin; Met: Methicillin; Van: Vancomycin. Source: Chakraborty et al. (2011) Isolation and identification of vancomycin-resistant Staphylococcus aureusfrom post-operative pus sample. Al Ameen J. Med. Sci. 4: 152-168. Vincent C. Okore 14
Susceptibility pattern of MRSA to some commonly used antibiotics Methicillin-resistant Staphylococcus aureus (n=30) Minimum inhibitory Minimum inhibitory Drugs concentration50 concentration90 Susceptible (%) Oxacillin >16 >16 0 Amoxacillin-clavulanate >16 >16 0 Ticarcillin-clavulanate >16 >16 0 Cefepime >16 >16 0 Ceftriaxone >16 >16 0 Imipenem >8 >8 0 Clarithromycin >8 >8 10 Gentamicin >16 >16 16.6 Amikacin >8 >8 16.6 Ciprofloxacin >2 >2 10 Teicoplanin 1 2 96.6 Vancomycin 1 2 100 Linezolid 1 2 100 Source: Calderon-James et al (2002) Epidemiology of drug resistance. Salud publica de Mexico 44: 108-112. Vincent C. Okore
Prevention/Reduction of Bacterial Resistance to Antibiotics • Rational Prescription/Use of antibiotics. • Non-systemic use of antibiotics for prophylaxis. • Rational use of antibiotics in veterinary medicine. • Surveillance and early interventions on the emergence of resistant bacteria. • Logical use of combined antibiotic therapies. • Use of inhibitors of bacterial enzymes that inactivate antibiotics, e.g. clavulanates, sulbactam, tozabactam, cepholothin, cephalosporidine, etc. Vincent C. Okore
References Afunwa, R. A., Odimegwu, D. C., Iroha, R. I. and Esimone, C. O. (2011). Antimicrobial resistance status and prevalence rates of extended spectrum beta-lactamase producers isolated from a mixed human population. Bosnian J. Basic Med. Sci. 11: 91-96. Calderon-James, E., Espinosa de los Monteros, L. E. and Avila-Betran, R. (2002) Epidemiology of drug resistance: The case of Staphylococcus and coagulase-negative staphylococci infections. Salud publica de Mexico 44: 108-112. Chakraborty, S. P., Mahapatra, S. K., Bal, M. and Roy, S. (2011). Isolation and identification of vancomycin resistant Staphylococcus aureus from post operative pus sample. Al Ameen J. Med. Sci. 4: 152-168. Shibata, H., Kondo, K., Katsuyama, R., Kawazoe, K., Sato, Y., Murakami, K., Takaishi, Y., Arakai, N. and Higuti, T. (2005). Alkyl gallates, intensifiers of β-lactam susceptibility in methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 49:549- 555. Vincent C. Okore