Download
1 / 82
850 likes | 940 Views
Coronary Heart/Artery Disease. J.B. Handler, M.D. Physician Assistant Program University of New England. CHD- coronary heart disease LDL- low density lipoprotein HDL- high density lipoprotein HTN- hypertension CAD- coronary artery disease PVR- peripheral vascular resistance

E N D
Coronary Heart/Artery Disease J.B. Handler, M.D. Physician Assistant Program University of New England
CHD- coronary heart disease LDL- low density lipoprotein HDL- high density lipoprotein HTN- hypertension CAD- coronary artery disease PVR- peripheral vascular resistance HCM- hypertrophic cardiomyopathy EF- ejection fraction PCI- percutaneous coronary intervention CHO- carbohydrate SVR: systemic vascular resistance (same as PVR) HF- heart failure CO- cardiac output CK- creatine kinase (also CPK) AIVR- accelerated idioventricular rhythm VT- ventricular tachycardia ACEI- angiotensin converting enzyme inhibitor T-PA- tissue plasminogen activator UF- unfractionated (heparin) STEMI- ST segment elevation MI vs NonSTEMI PAD- peripheral arterial disease PTCA- percutaneous transluminal coronary angioplasty Abbreviations
Coronary Anatomy AllRefer Health
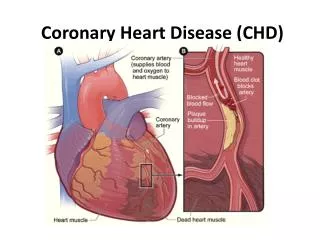
Atherosclerosis • Leading cause of cardiovascular disability and death in the U.S. More than 12 million persons have CHD and sequelae; 500,000 deaths/yr • Gradual process involving the 3 major coronary arteries and their branches: focal involvement. • Gradual reduction of arterial lumen resulting in ischemia due to reduced O2/blood supply. • Abrupt arterial occlusion/thrombosis initiates MI.
Coronary Atherosclerosis Images.google.com
Risk Factors for Atherosclerosis • Lipids: Total Cholesterol, LDL, HDL, triglycerides • Hypertension • Cigarette smoking • Diabetes Mellitus • + Family history for CAD- 1st degree relative- younger the onset, higher the riske.g. male <55; female <65.
Risk Factors for Atherosclerosis • Male gender • Age (men 45; women 55) • Hypoestrogenemia • Physical inactivity • Central obesity • Elevated plasma homocysteine levels • Amino acid derived from digestion of meat and dairy proteins • Elevation of CRP, an inflammatory marker
C-reactive Protein and Inflammation • A marker of chronic inflammation • Independent risk factor for CHD if elevated, even in patients with normal LDL-C. • Inflammation is likely a component of the atherosclerotic process • Chronic inflammation may be involved in the development of placque rupture and unstable coronary lesions. • <1 mcg/ml, 1-3 mcg/ml, >3 mcg/ml Intermediate risk Low risk High risk
Pathogenesis of Atherosclerosis: Endothelial Dysfunction • Chemical causes: LDL, homocysteine, glucose. • Hemodynamic- disturbed flow patterns, hypertension. • Biological- ??viral, endotoxin, immune complexes. • Nitric Oxide (NO) made by endothelial cells is protective: vasodilator with anti-atherosclerotic properties- decreased or absent production in presence of smoking, HTN and diabetes.
Prevention of Atherosclerosis • Primary prevention: Risk factor modification - smoking cessation, antihypertensive Rx, treatment of dyslipidemia, estrogen replacement (pre-menopause), glucose regulation/DM, regular exercise, aspirin prophylaxis in high risk groups. • Secondary prevention: Delay or abort disease progression in patients with documented CHD; more aggressive risk factor modification.
Aspirin and Primary Prevention • Emerging data using Aspirin and primary prevention of 1st MI (men), stroke (women) and vascular death. Physician’s Health Study data. • At risk: Men age 45-79 or women age 55-79 with 2 or more of the following risk factors: Smoking, HTN, hypercholesterolemia, +FH. • Diabetes: ASA for all adult diabetics with 1 other CV risk factor. • Recommendation: 75 ASA daily (optimal dose unclear). • Must balance gain from ASA against increased risk of bleeding.
Prevention and Lipids • Increased LDL increases risk of CAD, stroke and PAD. • Aggressive treatment can prevent coronary events and stroke in patients without clinically manifest disease (see lecture on dyslipidemias). • Secondary prevention – aggressive LDL lowering decreases progression and subsequent events in patients with documented atherosclerosis. • Disease regression unlikely, reported occasionally.
Coronary Artery/Heart Disease Images.google.com
Myocardial Ischemia • Coronary stenosis once significant, results in imbalance between blood supply and demand. This limits the normal increase in perfusion when there is increased demand (activity, exercise). • Contributory factors: myocardial O2 demand • Significant LVH, aortic stenosis) • Tachyarrhythmias (rapid Afib or flutter, others).
Effects of Active Ischemia • Symptoms usually present (below) but not always. • Cardiac: Mechanical, electrical and valvular dysfunction (mitral regurgitation). • Reversible vs permanent: dependent on how long ischemia is present; prolonged ischemia infarction. • Usually accompanied by characteristic ECG findings.
Silent vs. Symptomatic Disease • Long asymptomatic stage before symptoms. • Symptoms of reversible ischemia (angina pectoris) occur as a result of: • Increased myocardial O2 demand in the presence of fixed stenosis (supply) • Reversible decrease of O2 supply: vasospasm significant narrowing (with or without atherosclerosis) • Prolonged O2 supply often results in unstable angina or infarction. • Placque rupture and thrombosis likely present
Coronary Atherosclerosis NYerRN
Sudden Cardiac Death • Death within 1 hour after onset of symptoms; usually within minutes. Malignant arrhythmia commonly present. • Common presenting manifestation of CHD. • Frequent end point in patients with CHD, prior MI and impaired LV function. • 15-20% of patients with *AMI will die before reaching the hospital. *Acute Myocardial Infarction
Women are Different • Women with CHD often misdiagnosed; presentation often atypical: • Atypical symptoms: Unusual pain presentations • Pain radiating to right arm; arm pain alone • False negative stress tests common • Single vessel disease more common • Elderly or diabetic women: may complain of general malaise, loss of appetite, vague abdominal discomfort: if + risk factorsget ECG! • Need higher index of suspicion in women with risk factors.
Stable Angina Pectoris • Chest discomfort- heaviness, tightness, pressure, squeezing, burning, aching or choking; may not be described as “pain”. • Levine sign; substernal or to left of sternum. • Crescendo-decrescendo pattern, 1-5 min. • Radiation: left shoulder and upper arm, back, neck, jaw and teeth.
Precipitating Factors • Exertion, exercise, emotional duress, cold weather, sexual activity, cigarette smoke, large meals. • Patterns: Often reproducible with activity; patterns may vary depending on time of day, coronary tone; threshold lower in a.m. and after emotional duress. • Sx resolve with cessation of activity, relaxation and following sub-lingual (rapid acting) NTG.
Clinical Presentation • Characteristic history • Presence of risk factors • PE often normal in between episodes; may include: • Xanthelasma, xanthomas- hyperlipidemia. • Funduscopic abnormalities: A-V nicking, hypertensive, diabetic changes. • Cardiac- S4 gallop (during angina), bruits (atherosclerosis), murmurs, changes in BP.
Xanthelasma Images.google.com
Electrocardiogram • Often normal in between anginal episodes. May show prior infarcts, ST-T changes. • During episode may show characteristic ischemic changes: ST segment depression and/or T wave changes; changes normalize within minutes following an anginal episode.
Stress Electrocardiography • Most useful non-invasive procedure for evaluating the patient with angina. • Standardized protocols utilizing exercise or medications are used to increase cardiac workload (or coronary blood flow)- see lecture on cardiac testing. • Resting and stress ECG’s are compared looking for characteristic changes of ischemia.
Stress Electrocardiography Images.google.com
Stress Testing • Sensitivity/Specificity: Influenced by number of involved vessels, duration of exercise, and presence of resting ECG abnormalities. • Sensitivity/Specificity can be improved by adding imaging techniques: Myocardial perfusion scintigraphy or echocardiography- see lecture on cardiac testing.
Coronary Arteriography • The “gold standard” for assessing severity of CAD. Defines vessels involved, degree of stenosis and LV function. • Angiography is used in conjunction with patient’s symptoms and extent of ischemia (via stress testing) to determine severity and significance of disease, and is often the final piece of information necessary to determine therapeutic options.
Angiogram: Coronary Stenosis Images.google.com
Medical Treatment of Angina • Treat or eliminate aggravating factors. • Acute attacks: Sub-lingual NTG - venodilator>arterial dilator. Reduces LV volume (preload) decreasing O2 consumption; may improve collateral flow; also aborts coronary vasospasm. Usual dose is 0.3-0.6 mg, and repeated at 3 to 5 minute intervals. • Prophylactic sub-lingual NTG: taken 5 minutes before activities likely to precipitate angina.
Beta Receptor Blockers • Prevent angina by decreasing myocardial O2 consumption (MVO2); decrease HR, contractility and BP. Improve exercise tolerance and reduce symptoms. • Other benefits of ß-blockers: • Reduce mortality post MI • Reduce mortality in patients with heart failure (HF)
Beta Receptor Blockers • Can induce bronchospasm in patients with asthma or COPD: Role for ß-1 selective agents. • Numerous ß-blockers available. Choice may be influenced by selectivity and other features. Widely used in Rx of HTN, arrhythmias, HF, essential tremor and prevention of migraine headaches. • Propranolol, Atenolol, Metoprolol, Carvedilol, et al.
Long Acting Nitrates • Long acting nitrates- Oral, topical forms:Isosorbide dinitrate or mononitrate (oral)NTG ointment or patches (topical). • Used to prevent angina- MVO2;improve exercise tolerance. • Tolerance - need for nitrate free intervals. • Side effects: headaches, hypotension. • Must DC Viagra when using nitrates!
Calcium Channel Blockers • Decrease myocardial O2 requirements by dilating peripheral arteries/arterioles, reducing BP, LV wall stress, and afterload; also reduce coronary tone and spasm- induce vasodilation. • Result is MVO2 (myocardial O2 consumption) • Improve exercise tolerance/prevent angina • Some Ca blockers also have negative inotropic and chronotropic effects MVO2 • Do not reduce mortality post MI (compared to ß-blockers.
Dihydropyridine Ca Blockers • Dilate arterioles, PVR afterload MVO2Minimal negative inotropic and chronotropic effects. • Best used in addition to -blockers in the treatment of angina. • Long acting preparations reduce likelihood of hypotension. • Numerous available: Nifedipine, amlodipine, and others.
Diltiazem and Verapamil • Useful as an adjunct to nitrates in the treatment of angina (vs -blocker). • Dilate arterioles +HR and contractility MVO2. • Diltiazem can be used cautiously with -blocking agents in treatment of angina- avoid Verapamil. • Both are also useful in hypertension and for certain cardiac arrhythmias. • Avoid in patients with heart failure.
Ranolazine (Interest Only) • New (2006) for treatment of chronic angina in patients without adequate response to standard meds (above); modest improvement in Sx. • Unique MOA: s late Na current, ing intracelular calcium. Also decreases fatty acid metabolism,ing CHO metabolism which takes less energy/O2. • No significant effect on HR or BP. • Side effects: Dizziness, HA, constipation and nausea. • ECG: Increases Q-T interval; caution.
Anti-Platelet Agents • Low dose aspirin (81-325 mgs.) has been shown to reduce coronary events post myocardial infarction. Indications: all pts with CHD. • ’s incidence of subsequent MI, cardiac death. • Clopidogrel: inhibits ADP-induced platelet aggregation; option if ASA is contraindicated. • ASA or Clopridogrelalso recommmended in patients with PAD and carotid disease. • ’s incidence of subsequent MI, cardiac death, stroke.
Revascularization: Indications • Patients with unacceptable symptoms in spite of optimal medical Rx. • 3 Vessel CAD especially with LV dysfunction • Left main or left main equivalent disease • Following treatment of unstable angina if there is evidence of early onset ischemia. • Patients post MI with ongoing ischemia, or with early onset ischemia via stress testing. • Acute MI (see below) CABG
Catheter Based Techniques • Angioplasty and related techniques can be performed with low morbidity, mortality, and rapid recovery. • Indicated primarily for single or 2 vessel disease. • Comparable mortality and infarction rates compared to CABG over 1st three years, but high rate of repeat procedures until recently. • Major drawback: Restenosis requiring repeat/multiple procedures improved last 5 yrs with newer drug eluting stents (below).
Catheter Based Techniques • Catheters used to open stenosed/occluded coronary arteries or bypass grafts. • Angioplasty (PTCA), Atherectomy, etc. • Problem: 30-40% re-stenosis rate. • Stent Placement- insertion of metal “sleeve” into stenosis: re-stenosis-15-20% • Using drug eluting (Sirolimus, Paclitaxel) stents ’s re-stenosis- 5-8%: problems with late stent thrombosis intense anti-platelet Rx..
Coronary Angioplasty Images.google.com
Coronary Angioplasty and Stent Images.google.com
Stent Placement Images.google.com
Coronary Artery Bypass Surgery • Obstructed coronary arteries are bypassed using veins or arteries. Low mortality (1-4%) if LV function preserved. • Best long term results of patency and flow. • Saphenous veins, radial artery and internal mammary arteries are commonly used to bypass diseased segments.
Coronary Bypass Graft Surgery Images.google.com
Coronary Artery Bypass Surgery • Operative mortality increased if age > 70, EF< .35. • Vein closure rates: 10-20% in 1st year, then 4% annually; vein grafts and native vessels subject to recurrent disease. • Internal mammary grafts-high patency rate over time- best option for grafts where possible. • Radial artery grafts are better than vein grafts, but use is limited.
Coronary Vasospasm • May present in patients with normal coronaries, or superimposed on atherosclerotic disease. • Often induced by exposure to cold, emotional stress, meds (ergot), or drugs (cocaine). • Clinical presentation: Chest discomfort accompanied by ST segment elevation and arrhythmias. • May progress to MI (and consequences) if spasm does not resolve.