Download
1 / 54
540 likes | 650 Views
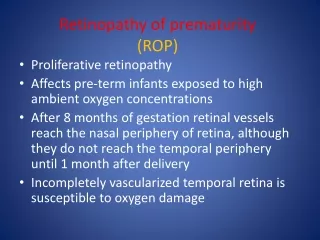
Impact of Best Evidence on the Management of ROP. Dale L. Phelps, MD University of Rochester, NY Israel Neonatology Association The Dead Sea, Dec. 14- 15 , 2006. Case Report. 780g male, 25 weeks RDS & BPD, sepsis x1, PDA, ROP 4 ROP exams prior to discharge at 36 weeks

E N D
Impact of Best Evidence on the Management of ROP Dale L. Phelps, MD University of Rochester, NY Israel Neonatology Association The Dead Sea, Dec. 14-15, 2006
Case Report • 780g male, 25 weeks • RDS & BPD, sepsis x1, PDA, ROP • 4 ROP exams prior to discharge at 36 weeks • Next exam due Aug. 1, discharged Jul.31(Sat.). Instructed to call for appointment Mon. • Called MD Mon., given appointment for 8/23 • Bilateral retinal detachments when seen • … Effective treatment depends on timing
Evidence and Practice • Newer Oxygen Story • Can we Prevent ROP otherwise? • Data on Treatment of threshold • (Screening) Detecting Serious ROP • Follow up of ROP
An RCT of Transcutaneous Oxygen Monitoring • Continuous TcO2 monitor while on any O2 • vs Intensive TcO2 only when acutely ill • n= 296, 500g-1300g birth weight • No significant differences • any ROP: 51.0% vs 59.0% • Cicatricial ROP: 4.0% vs 4.4% Bancalari, Flynn, et al Pediatrics 1987;79:663
An RCT of Transcutaneous Oxygen Monitoring • Secondary analysis: • Continuously Monitored Group • For each 12 hrs of time from birth to 4 weeks that Tc-PO2 was over 80 torr, • odds ratio for ROP increased 1.9 • In weeks 2 through 4, for each 12 hours that the Tc-PO2 was over 80 torr • the odds ratio was increased 3.1 Bancalari, Flynn, et al Pediatrics 1987;79:663
UK- Results from Differing Pulse Oximetry NICU A Stated Pulse Oximetry Goals 88-98% NICU B 70-90% Tin et al, Arch Dis Child Fetal Neonatal, 2001;84:F106-10
Infants <28 weeks 1990-1994 Tin et al, Arch Dis Child Fetal Neonatal, 2001;84:F106
Reduction in Rates of ROPAn Historical Comparison-USA • BW 500-1500g • Rates of stage 3 or worse ROP • Pre-intervention 1997 • Intervention 1998 forward • Delivery Room: blender and saturation monitor • NICU: proportional response, prompt weans • Target saturations: 85-93% Chow, Sola, et al, Pediatrics 2003;111:339
Laser Treatment of ROP Chow, Sola, et al, Pediatrics 2003;111:339
Seymore(see-more) Ochsner, with permission: NICU, New Orleans
Oxygen Targeting: Effect of New Targets on % Time at Certain Saturation Ranges 100 Old Target: 90-100%, Alarm at 85% No upper alarm New Target: 85-93%, Alarm at 80-95% 90 80 70 60 50 % Time at Saturation 40 30 Old Target 20 New Target 10 0 60 70 80 90 100 O2 Saturation Ochsner, with permission: NICU, New Orleans
Contract Summary birth weights 500-1500 g 1. Set saturation alarm limits at 80-95%. 2. Goal of saturations to be 85-93%. 3. Allow baby to fluctuate 5. Never increase the FiO2 without first assessing the baby. 6. When altering oxygen, stay until saturations are stabilized within an acceptable range Summarized from Ochsner: New Orleans
% Stage 3-4 ROP in <1500 gm Ochsner, with permission: NICU, New Orleans
Individual Nurse Performance in Titration of O2 to Prescribed SpO2 Ranges Ochsner NICU: New Orleans
Oxygen Delivery • Not just saturation • Cardiac Output • Hemoglobin • Hemoglobin Oxygen Affinity • Growth is modified by oxygen delivery as well a nutrient delivery: together William Hay, Denver, Colorado
International Pulse Oximetry Studies Beginning • Primary Outcome • Neuro-Development at 2 yrs • Secondary Outcome • Survival without ROP requiring Surgery • (or meeting criteria for surgery)
ROP--pulse Oximetry Trials • Target Saturations 85-89% vs 90-95% • double blind RCT, with research Oximeters • Orders: “Maintain saturation 88-92%”
Normal Term Normal in utero 60-75 % SATURATION Target Ranges in the Oximeter Trials PaO2 20 40 60 80 100 120 2
Evidence and Practice • Newer Oxygen Story • Can we Prevent ROP otherwise? • Data on Treatment of threshold • (Screening) Detecting Serious ROP • Follow up of ROP
Preventing ROP • Prevent Preterm Birth • Birth intervals at least a year • 17-OH progesterone • Manage Oxygen Wisely • Others? • Light, Vitamin E, Inositol, d-penicillamine
Restricting Light (Cochrane) • 3 Randomized Controlled trials with n= 184, 127, and 409. • Patching or high density goggles from birth to ~34 weeks • No evidence that ambient light affects the incidence or severity of ROP Cochrane Review: Phelps and Watts • May be other reasons than ROP to limit light exposure
Vitamin E to Reduce ROP • One Systematic Review 6 RCTs summarized • n = 1428 infants, 704 Vit E prophylaxis • Any ROP: 43% vs 40% (vit E) • Stage 3+ ROP: • pooled odds ratio 0.44 [0.21-0.81, 95% CI] • Number Needed to Treat = 35 • Recommended further, focused trials • (Raju, J Peds 1997;131:834)
Inositol to Reduce ROP • Hallman: 2 RCTs with IV Inositol • n = 74, n = 221 • Outcomes: Relative Risk [95% confidence interval] • Death RR 0.48 [0.28, 0.80] • Death or BPD 0.56 [0.42, 0.77] • Severe ROP 0.09 [0.01, 0.67] See Cochrane Review: Howlett, A, 2000
MulticenterRCT FundedInositol to REDUCE ROP • Infants of <28 weeks gestation • double blind, placebo controlled • Primary Outcome survival without meeting criteria for Surgical ROP • Pilot Studies on pharmacokinetics in extremely preterm are enrolling Phelps DL, & NIH Neonatal Research Network
d-penicillamine to prevent ROP • Two RCT reported by Lakatos • n=204, 750-2000g birth weight • Acute ROP in 0/71 penicillamine vs 6/70 control survivors • n=77, 751-1500g birth weight • Acute ROP in 0/27 penicillamine vs 3/22 controls • to be continued… Trials needed Phelps et al, Cochrane Review 2001
Evidence and Practice • Newer Oxygen Story • Can we Prevent ROP otherwise? • Data on Treatment of threshold • (Screening) Detecting Serious ROP • Follow up of ROP
CRYO-ROP: 15 Years • Controls Worse % poor Control Good News: Something we can do ! CRYO Bad News: Something we can do ! but doing it is not easy. Arch Ophthal 2005; 123:311
ETROP Study • Earlier Treatment • Prethreshold that was “High Risk”, • meant a >15% chance of poor outcomes • Used Laser • Zone I more common Arch Ophthal 2003 121:1684
ETROP Outcomes Percent Poor Retinal Outcomes P<0.001 15.6 9.1 Arch Ophthal 2003 121:1684
Revised Indications for ROP Modified from: Arch Ophthal 2003 121:1684
Surgery for Stage 4b or 5 ROP • Vitrectomy /lensectomy • Outcomes disappointing at best • Rarely: ambulatory vision, usually none • 72 eyes receiving vitrectomy from the CRYO-ROP study: 1 with pattern vision at 5 years, otherwise no LP or just light perception • Devastating to Families who reach for any hope, and often give all they have • Neonatology should counsel too, separate perspective Ophthal 1996; 103:595
Progression to Retinal Detachment Stage 4a Stage 4b Stage 5 Arch Ophthal 1987; 105:906, used with permission
Surgery for Stage 4A ROP • Partial Detachment, not macula • From CRYO-ROP, condition documented as unstable • Surgery is not established treatment, but is being attempted: • A vitrectomy (with lens sparing, or with lensectomy), done as soon as any detachment is seen • Watch for the data (outcomes)
Evidence and Practice • Newer Oxygen Story • Can we Prevent ROP otherwise? • Data on Treatment of threshold • (Screening) Detecting Serious ROP • Follow up of ROP
Screening for ROP Goal: Detect New/Threshold ROP in time to treat it
Screening for ROP (2) • Who to examine? • When to start exams? • When to repeat exams?
2006 USA Guidelines Who? • Note: Varies by Country • Who? • <31 weeks gestation (i.e. 30 and less) • <1500 grams birth weight • other premature infants, if medically unstable
Who are: “Other Preterm, Unstable” Babies ? • 310/7 to 360/7 weeks • If hypotensive (pressors, volume, steroids) • If on oxygen more than 6 hours • If culture proven septic (early or late) • Exchange Transfusion • Small for Gestational Age • Others as judged by physician
Recommended First Examination Range 31-33 weeks Timing of Threshold ROP Youngest, 31.6 weeks
When to Start Exams? • 31-33 weeks PMA official • Because in ETROP, High Risk Prethreshold occurred at • mean 35.2 weeks, • range 30.6-42.1 weeks • Consider • Targeting 31 weeks PMA
Recommended First Examination Range 31-33 weeks Mean ETROP threshold ETROP Type 1 ROP Youngest now 30.6 weeks
When to Examine GA PMA Postnatal Age at birth at exam at exam . 24 weeks 31 weeks 7 weeks 25 31 6 26 31 5 27 31 4 28 32 4 29 33 4 30 34 4 31 35 4* * OK to do the exam before discharge 32 36 4* home, if sooner. This is because if the 33 37 4* retinalvesselsare mature by then, no 34 38 4* further exams are needed asan 35 39 4* outpatient. 36 40 4* Modified from Reynolds: Arch Ophthal 2002 120:1470
When to Repeat Exams ? • Confer with Ophthalmology • Your population • Monitor it • If Type 2 ROP (watch and wait) • Examine every 2-4 days (twice weekly) • Close to Type 2, ? Weekly • (only prethreshold used to be weekly) • Zone I, no ROP • Zone II, stage 2
Recommended First Examination Range 31-33 weeks Mean Time for ETROP threshold Discharge Home ETROP Type 1 ROP Youngest now 30.6 weeks
Tracking for ROP Must be a Collaborative Policy with Neonatologists, Ophthalmologists & Pediatricians We work hard on these Policies Ask: Have you done a QA on its effectiveness?
Testing Effectiveness in your NICU • Test a 6-12 month period • List all births <1500g or <=30 weeks • Determine final outcome of each • Death • Was ROP status “final” before discharge? • Death, mature, regressed, zone III x2 • If not, did parents return for timely and complete follow-up?
Evidence and Practice • Newer Oxygen Story • Can we Prevent ROP otherwise? • Data on Treatment of threshold • (Screening) Detecting Serious ROP • Follow up of ROP
2 Kinds of Ophthalmic F/U • Urgent-Immediate Follow-up • Goal: Prevent Blindness • Window: Days to Weeks !!!! • Ongoing Ophthalmic Care • Goal: Optimize Vision • Window: Months to Years
Discharge Planning and ROP • Schedule Appointment before discharge • Letter with appointment, phone numbers and signature of family • Copies to home, medical record, ophthalmologist’s office • If very close to ROP treatment, consider delaying discharge
Pediatrician Role • Understand it is sometimes Urgent • Ask family about ROP, and ask at discharge • Insist family attend follow up appointments • Don’t be afraid to say ‘blind’, and that treatment might prevent it.