Download
1 / 67
670 likes | 798 Views
HEPATITIS C VIRUS. Structure of presentation. HCV epidemiology,viral dynamics,immunopathogenesis,diagnosis HCV renal disease, management HCV in CKD,CKD5D,CKD5T KDIGO guidelines. by the late 1970s it was apparent that HBV was not the only cause of "serum" hepatitis,

E N D
Structure of presentation HCV epidemiology,viral dynamics,immunopathogenesis,diagnosis HCV renal disease, management HCV in CKD,CKD5D,CKD5T KDIGO guidelines
by the late 1970s it was apparent that HBV was not the only cause of "serum" hepatitis, • and that other "non-A-non-B" hepatitis viruses existed , which • could be transmitted by blood products to humans and chimpanzees
Houghton and colleagues cloned and expressed portions of a RNA virus from the plasma of an infected chimpanzee in 1989 • This virus, designated hepatitis C virus (HCV), is now known to be a major • cause of both transfusion-associated and sporadic non-A-non-B hepatitis
The persistent and indolent nature of HCV infection often • results in prolonged viremia in spite of a strong humoral immune response
To date, around 170–200 million individuals worldwide are estimated by the WHO to be chronically infected with HCV.
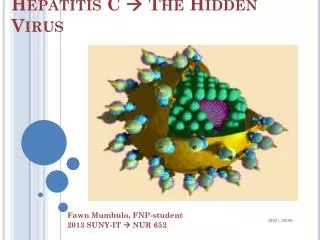
THE VIRUS…… • Flavi virus • 50 nm particles • Nucleocapsid • RNA • Envelope • Circulates…. a. lipo-viro-particles b. Ig bound c. free virions
The genome • RNA with 9600 nucleotides,encoding 3010 aminoacid polyprotein • Single polypeptide • Structural and non-structural 1. core – steatosis , IFN resistance 2. E1,E2 – cell entry 3. p7 – viral maturation & release 4. NS2 – autoprotease 5. NS3 – serine protease & helicase 6. NS4a – cofactor for 5 7. NS4b – membranous web for replication 8. NS5a – RNA binding , steatosis , 9. NS5b – RNA dep. RNA polymerase 10. IRES – internal ribosome entry site
Significant nucleotide and amino acid heterogeneity is present throughout the HCV genome, with a well characterized • hypervariable region in the E2 envelope glycoprotein domain . • This has led to the recognition of at least six HCV subtypes based on differences in the nucleotide sequence for NS5 .
Infection is followed by an incubation period of 6 to 12 weeks prior to the development of clinical hepatitis. • In the majority of cases the hepatitis is mild and anicteric. Persistent viremia despite resolution of the acute hepatitis is seen in the majority of cases. • many of these patients have persistent viremia despite minimal liver pathology, suggesting the presence of a "healthy“ carrier state, • at least 50% of patients develop chronic hepatitis, of which 20% progress to cirrhosis or chronic active hepatitis
Genotype… • Genetically distinct groups of HCV isolates arisen during viral replication • 35% variation esp. E1 E2 Distribution 1 --- 40 – 80% worldwide 1a – USA ; 1b – Europe 2 --- 10-40% worldwide 3 ---- India , Australia 4 --- Middle East , Africa 5 --- South Africa 6 --- Hongkong • Do not influence severity • Treatment response • Genotype 3 – steatosis • Genotype 1b – progressive post transplant disease
Quasispecies… Closely related heterogeneous sequences in HCV in single infected person Mutation on replication E1E2 HVR Escape host immunity Resistance to treatment
EPIDEMIOLOGY • Seroprevelance • Worldwide : 3% (Range 0.1 – 26%).Highest – Egypt • India : 5% (Intermediate) • Voluntary blood donor 0.6 – 0.8 % • Gen.Population 1.8% • Sex M: F 2.5 : 1.2
Epidemiology • Epidemiology patterns • Peak prevalence (Age) 30-50 yrs Recent source 1980-1990 IDU • Peak prevalence > 50 yrs Remote acquisition 30 yrs ago • Unsafe injections • Folk medicine
Transmission • Percutaneous • Blood transfusion • Needle stick • Non percutaneous • Sexual • Perinatal
Transfusion • Initial Post Transfusion hepatitis : 85% Hep C • Transfusion Hep C – 4% of Acute HCV • Decreased after anti-HCV introduced in May 1990 • Present risk - 0.01 – 0.001 % • At risk • Patient Requiring multiple transfusions • Hemophilia • Thallasemia • Apollo chennai - HCV in blood donors : 3-5/ year (14,000 donations) • HCV RNA screening
IDU & others… Prevalence : 48 – 90% More than HIV & HBV Positive in 6 months Tattooing – 2- 24% Acupuncture
Hemodialysis • Anti HCV prevalence: 10- 20% • Underestimate (4-15%) • Duration on HD • Annual Risk : 0.15% (HD) & 0.03% (CAPD) • Chr.HCV : 70-90% At Apollo • HCV+ve on HD – 11/140
HCV in CKD on HD • Prevalence – 1. Developed nations – 7 – 40% 2. Developing nations– 16 – 80% 3. India – 12 – 40% ( Saha etal 2001) 4. Apollo – 12% • Risk factors – 1. Duration on HD 2. Local prevalence 3. Blood transfusions 4. Nosocomial transmission November 17, 2014 HCV and Renal Disease
Nosocomial Transmission… • Breach of standard infection control precautions 1. Hand wash , glove change Okuda et al ; Arenas et al 2. Multi-dose vials 3. Spillage • Dialysis internal circuits minor contributor • DOPPS – Isolation does not protect • CDC – 1. No isolation 2. No dedicated machines • Belgian study – 0% transmission by standard precautions only • Slow seroconversion ( 5 months) • Regular EIA / NAT , ALT / AST November 17, 2014 HCV and Renal Disease
Nosocomial • Health workers • Needle stick : 0-4% by anti-HCV 10% by PCR • Overall seroprevelance is as gen.population • Risks of transmission < HBV,HIV • HCW patient 0.014% • Patient HCW 2- 10%
Non-percutaneous Sexual – controversial More common in male homosexuals Associated risk factors RNA levels in semen low HCV in spouse 3%
Perinatal Transmission • Risk upto 10% • No difference in CS vs. vaginal • Increased risk • RNA +ve • Increased RNA levels • HIV-HCV decreased with HAART • Not transmitted by breast feed • Passive transfusion of Anti HCV • Anti HCV upto 18 months
Sporadic HCV Upto 30- 40% of cases Occult / unidentified percutaneous Sharing of hygiene items Forgotten risks, Transfusion Multi-dose vials Cocaine snorting
Pathogenesis • Viral • Human • Environmental Main sites : Hepatocyte Other : Mononuclear : Dendritic cells
Immune Mediated Mechanism • Humoral Response • CMI • CD4 • CD8 - liver infiltrating • NK
CMI Response • CD4,CD8, NK • Protective and Destructive • More in Acute cases • Activated by antigen presentation • CD4+ (polyclonal) TH1 TH2 • TH1 IFN + IL2 NK cells & CTLs • TH2 IL4 + IL10 decrease TH1 • TH1 viral clearance
Viral persistence • Quasi-species nature • Immune evasion • Inadequate innate immunity • Insufficient adaptive response • Re-infection with different strain
Pathogenesis.. • Pathogenesis - Viral - Host - Environmental
Viral • Direct cytopathic effect • Viral Protein • Viral particles • Steatosis 30 – 70% • C, NS5a viral proteins • Genotype 3 • Activation of lipid peroxidation • Increased RNA Increased Steatosis • Contribution of fibrosis - Oxidative stress - Hyperinsulinemia
CMI in pathogenesis…… CD8+ Polyclonal activation Increased in infected liver IFN gamma Hepatocyte cytolysis Inhibit multiplication
Humoral immunity…… • Ig to viral proteins • Non neutralising • 4 – 8 weeks of infection • Marker of infection • Lymphoid aggregates • Extra hepatic manifestations B cell ++ polyclonal Ig auto Ig • CD5 ++ rheumatoid factor cryoglobulinemia ( Ig + RF )
Summary of Pathogenesis • Viral replication & persistence • Inhibition of innate immunity • Balance between CD4 & CD8 hepatocyte damage • Poor response in chronic disease • Viral cytopathic effect • Antibodies --- 1. diagnostic 2. extra hepatic manifestations
Extrahepatic manifestations • Mixed Cryoglobulinemia • MPGN • Porphyria cutanea tarda • NHL • Leucocytoclastic vasculitis • Focal lymphocytic sialadenitis • Lichen planus • DM • Rheumatoid arthritis • Thyroid disease • Non specific antibodies ANA – 20% , ASMA -20% , anti LKM – 5% , cryoglobulins-40%
Mixed cryoglobulinemia • Circulating Igs precipitating at < 37c • Vasculitis by deposition of cryoprecipitate in small vessels • IgG, IgM RF, anti HCV, HCV RNA , LDL • IgM RF from liver • B cell activation by E1 E2 – CD81 interaction • 50 -90% EMC – HCV + • 60% HCV pts. - MC (30%asymptomatic) • Purpurae, arthralgias , weakness • Peripheral neuropathy • Raynaud’s phenomenon • MPGN – nephrotic syndrome liver disease occult • Antiviral therapy
Extrahepatic manifestations…. B cell NHL – HCV 15% lymphotropism & clonal expansion Sialadenitis – 10% patients Diabetes Mellitus – steatosis , insulin resistance,
In a nutshell…. • A RNA virus with hepatotropism • Widely distributed with distinct genotypes • Evades immune system • Pathogenesis by steatosis fibrogenesis & host immunity • Transmission by parenteral route • Acute hepatitis rarely recognised • High rate of chronicity • Multiple influences • Extrahepatic manifestations • HCC
Mesangio proliferative gn • igA • Fibrillary and immunotactoid gn • Diffuse endocapillary proliferative gn • MGN • MPGN • Renal vasculitis cryoglobulinemic
HCV induced renal disease • EMC type II ( 50% of HCV ; 1% symptomatic) • MPGN type I ( with or without MC) • Membranous glomerulonephritis • Pathology - Deposition of HCV RNA – Ig complexes • OLT – intraop renal biopsy – 25 – 30% GN • Proteinuria , Microscopic hematuria • Liver disese may be occult • Melzer Franklin triad (EMC) Weakness , Arthralgia , Purpurae Elevated Cryocrit ,Rheumatoid factor ; Decreased C4 • Test annually 1. hematuria 2. proteinuria 3. GFR • Renal biopsy November 17, 2014 HCV and Renal Disease
Diagnostic tools… • Serological 1. Enzyme Immunoassay (EIA) 2. Recombinant Antigen Immunoblot Assay (RIBA) • HCV RNA detection a. Qualitative b. Quantitative Methods 1. PCR 2. TMA (Transcription mediated amplification) • HCV Genotyping • Liver biopsy
Serological…… • Detect Igs against viral proteins • EIA 3rd generation • NS3 , NS4 , NS5 • Positive at 7 – 8 weeks • Sensitivity – 97% • RIBA for clarifying false positives • Negative anti- HCV in HCV infection 1. immunosuppressed 2. CKD , on HD 3. Acute HCV
The original first generation enzyme immunoassay (EIA-l), which measured antibodies to the nonstructural Cl00-3 antigen (coded by the NS4 domain), lacked sensitivity and specificity, and was undetectable in 10 to 25% of patients with chronic HCV viremia and falsely present in both healthy individuals and patients with chronic autoimmune hepatitis
The second generation enzyme immunoassay (EIA-2) measures antibodies to recombinant core and NS3 antigens in addition to that coded by NS4, and has greatly improved sensitivity (—95%) and specificity. • A supplemental serologic assay, the recombinant immunoblot assay (RIBA II test), measures antibody to four HCV antigens (the nonstructural antigens 5-1-1, C100-3, and C33, and the core antigen C22), and has comparable sensitivity and slightly more specificity than the EIA-2 test