Download
1 / 18
180 likes | 304 Views
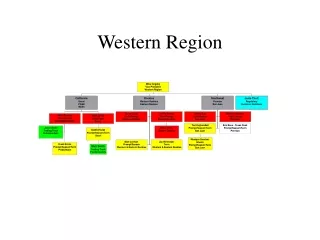
Child Nutrition In the West 2001-2003 Western Region Health Centre. Child Nutrition in the West. Key program areas : 1. Bilingual Peer Education 2. ‘Fresh Kids’ - c reating healthy eating environments in six Maribyrnong primary schools

E N D
Child Nutrition In the West2001-2003Western Region Health Centre
Child Nutrition in the West Key program areas: 1. Bilingual Peer Education 2. ‘Fresh Kids’ - creating healthy eating environments in six Maribyrnong primary schools 3. Development of the Vietnamese child nutrition resource
Promoting daily fresh fruit, vegetables & water in schools Fresh Kids Fruit break everyday in class Partnerships with wholesalers Water bottles (Moonee Valley Child Nutrition Partnership) Nutrition curriculum Bilingual nutrition education for parents Fruit & water policies
Bilingual Peer Education The essence of Peer Education is to share ownership of information and the ability to communicate that information to peers
Program context • Forty nine percent of Maribyrnong population born overseas • Traditionally dietary education has an illness focus • Facilitated by Dietitians with interpreters during health centre business hours
Bilingual Peer Education • Recruited 12 local women from 6 language groups • Nine training days over five weeks. • Five days ‘Child Nutrition’ developed by Dietitian. • Four days training skills facilitated by CAE: Nationally Accredited Certificate IV Assessment and Workplace Training Course • Employed by WRHC to facilitate formal nutrition education • Ongoing individual & group support by WRHC Dietitian
Nutrition education themes • General healthy eating • Promoting breast feeding & safe bottle feeding • Introducing solids for infants • Managing fussy eating for toddlers • Why no sweet drinks for infants & toddlers • Nutrition for pregnant and breastfeeding mothers • Preventing Vitamin D deficiency • Preparing school lunches
Impact • Over eighteen months 12 BNE have delivered 78 nutrition education sessions to over 850 people from linguistically diverse communities. • Increasing access to education through existing community networks: schools, mosques, churches, housing estates, migrant resource centres & SBS radio • Increased confidence, knowledge and skills for BNE.’.. our families are eating better now’ • Successful trial of a new model in community health nutrition
Contextual factors that made a difference • Commitment & enthusiasm of individual educators • Providing employment opportunities • WRHC management support to reorientate traditional dietetic services • Dietitians breaking down professional boundaries • Collaboration & partnership between agencies
Community engagement BNE successfully engaged their communities by: • Dual employment of educators • Power of word of mouth • Knowing how to get the message across • Sharing culture, language & experience • Understanding the diet & lifestyle transition upon re-settlement • Understanding traditional beliefs around food & health • Peers as positive role models
Promoting better access to nutrition education Shared language powerfully integrates mutual understanding of gender, race, history and experience ‘…Peer education is a sharing of experience so they don’t expect me to have qualifications. My community would respect any professional person trying to help, but they would just listen and not ask questions and they would probably just go away and not do anything about it ..’ .
Project sustainability Facilitators • Integration within WRHC Health Promotion Strategic plan, Neighbourhood Renewal, Best Start • Dual employment of five educators • Accredited training component • Transference of the peer education model to other health areas • Ongoing relationship of BNE within existing community networks
Informal learning ‘When they see me in the supermarket they come and look in my trolley and ask questions about the things that I buy’ ‘I go to my friends houses and I know longer see soft drinks in their fridges, just juice and water’
Project sustainability Barriers • Funding required to continue employment • Need for Victorian public health nutrition policy to sustain local projects • Insufficient public health nutrition workforce • Increasing access & intense promotion of food/drinks of poor nutritional value targeting children
‘In our country many generations have grown up healthy eating the same way.’ Once arriving in Australia the educators reported that often the participants of their sessions would not understand the language spoken in advertisements… ‘they just see kids having fun at McDonalds in the advertisements and sometimes they think that their kids will be happier if they feed them from there.’
Evaluation • External Evaluation: Deakin University facilitated two focus groups with Bilingual Nutrition Educators to identify • community nutritional beliefs and concerns • quality of training and support • administration of the program • impact of nutrition education sessions • value of peer education verses health professional education • Internal evaluation: participant evaluation via telephone surveys & written surveys
Example of internal evaluation • Results of eight telephone interviews using Vietnamese Interpreter after completion of five sessions with Linh Nguyen • 50-70% new information for all attendants • ‘After the sessions I change to feed my son meat & fish moderately. Before I listened to my friends I fed him plenty of meat. I also increase meals and give him less bottles’ • ‘Before I eat everything I like but now I choose and balance my food intake which has the five food groups’ • ‘I give her cheese now and I do not give her soft drink and chips as much as I can’ • I advise them not to drink much soft drink. Drink more water • I have more knowledge about what food to give my child and how much he needs instead of forcing him to eat the meat before
Next time • Maximise the value of peer education through linkages with broader public health nutrition programs, eg Fresh Kids. • Encourage nutrition education in a series of sessions • Greater promotion of BNE • Greater focus on food preparation utilising community kitchens • Engage school aged children with parents in nutrition education