Download
1 / 18
180 likes | 214 Views
Low Grade Lymphomas: Treatment approaches. Parameswaran Venugopal, MD Professor of Medicine Rush University Medical Center. SEER DATA 2015. SEER DATA 2015. Relative Incidence of NHL Subtypes. Armitage and Weisenburger. J Clin Oncol. 1998;16:2780.

E N D
Low Grade Lymphomas:Treatment approaches Parameswaran Venugopal, MD Professor of Medicine Rush University Medical Center
Relative Incidence of NHL Subtypes Armitage and Weisenburger. J Clin Oncol. 1998;16:2780. Adapted from Jemal et al. CA Cancer J Clin. 2006;56:106.
Selected Indolent B-Cell Non-Hodgkin’s Lymphoma Subtypes *%of all NHL. National Comprehensive Cancer Network. Practice Guidelines in Oncology. v.2.2006. At: http://www.cancer.gov/cancertopics/pdq/treatment/adult-non-hodgkins/HealthProfessional/page2. Accessed May 2006. Ansell and Armitage. Mayo Clin Proc. 2005;80:1087.
Indolent lymphoma accounts for 30%-40% of NHL cases FL (22%), SLL (7%), MALT (8%), WM (uncommon) Often asymptomatic 85%-90% present in stage III or IV (Ann Arbor Staging) Long median survival (~10 years) Advanced disease rarely curable with conventional treatments Transformation to aggressive lymphoma often occurs 3% risk/year 30% risk over 10 years Low Grade Lymphoma Winter et al. Hematology. 2004;203. Armitage and Weisenburger. J Clin Oncol. 1998;16:2780. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10. Al-Tourah et al. ASCO, 2006. Abstract 7510.
Follicular Lymphoma (FL) • Most common indolent NHL, accounts for ~22% of NHL in North America • Typically advanced stage at presentation • Often asymptomatic
FL: WHO/REAL Grading Grade 1 <5/hpf Grade 2 Grade 3a 6-15/hpf Grade 3b >15/hpf Sheet
Follicular Lymphoma: Diagnosis • B symptoms • Physical Examination • Laboratory studies: • Biopsy of Lymph Node • Bone Marrow Biopsy • CAT Scan • PET scan
Watch & WaitRadiotherapyChemotherapyMonoclonal AntibodiesRadioimmunotherapyStem Cell TransplantationNew Agents:
New Agents: Ibrutinib (Imbruvica) Idelalisib (Zydelig) Venetoclax (Venclexta) Obinutuzumab (Gazyva)
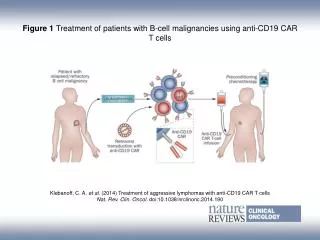
Murine/human IgG1 kappa monoclonal antibody Binds to CD20 antigen Half-life (at 375 mg/m2) ~76.3 hours after 1st infusion and 205.8 hours after the 4th infusion Mechanism of action CDC, ADCC, apoptosis, and ionizing radiation–induced cell death Rituximab as a Targeted Therapy in FL Murine variable regions bind specifically to CD20 on B cells Human constant regions Human IgG1 Fc domain works in synergy with human effector mechanisms CDC = complement-mediated cell death; ADCC = antibody-dependent cell cytotoxicity.
Granules Fc receptor (FcgRIII) Antigen Fc region Antibody NK cell B cell Granules release perforins and granzymes; cytokines secreted (eg, IFNg) Lysis H2O, ions, granzymes Pores (perforin) Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC) NK = natural killer.
Radioimmunotherapy Ibritumomab Tositumomab Chelator Radionuclide Tiuxetan
Targeting of B Cell Receptor Niedermeier M, et al. Blood. 2009;113(22):5549-5557.