Download
1 / 64
660 likes | 882 Views
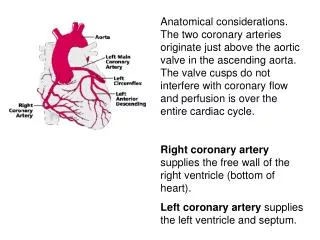
Coronary blood flow (CBF) Resting rate about 1 ml/min/gm . Thus for a 200 gm human heart coronary flow would be about 200 ml/min or ~5% of the cardiac output. It is always in an active hyperemia because the heart is a working muscle. Coronary blood flow (CBF)

E N D
Coronary blood flow (CBF) Resting rate about 1 ml/min/gm. Thus for a 200 gm human heart coronary flow would be about 200 ml/min or ~5% of the cardiac output. It is always in an active hyperemia because the heart is a working muscle.
Coronary blood flow (CBF) High degree of oxygen extraction at rest. 95% of the oxygen is extracted from the coronary blood on a single pass vs. ~ 75% for the rest of the body. • Metabolism is primarily by beta oxidation of FFA. • Glucose oxidation accounts for only about 15% of metabolism. Knocking out long-chain acyl-COAa synthetase -1 blocks lipid metabolism in the heart by animals have a near normal phenotype except for increased mitochondrial content.
Notice the reactive hyperemia following the occlusion. Theheart requires a continuous metabolic supply. Only 10 sec of coronary artery occlusion causes a marked drop in contractility. If continued the ventricle would be akinetic in 60 seconds Reason for CPR
Oxygen is the rate-limiting metabolite in ischemia. During ischemia anerobic glycolysis of glycogen and glucose continues but at too low a level to maintain viability. Blocking glycolysis with iodoacetate hastens cell death showing that glycolysis is nutritional
It is not known exactly why the contractility falls so quickly in ischemia. • Thought to be a mechanism to conserve ATP. • H+ competes with Ca++ at the troponin binding sites but this accounts for only a small fraction of the depression. • Accumulation of Pi are also thought to inhibit contraction
While contractility falls quickly, cell death doesn’t start until ~20 min after the onset of coronary occlusion and then progresses over the next 6 hr (dog measurements – human heart is probably much slower). Often the occlusion involves only a small branch and the heart will continue to pump blood normally. If the region can be reperfused quickly the ischemic region can fully recover.
Three Factors Control CBF • Mechanical. With each beat thecontracting heart muscle pinches the coronary arteries and increases their resistance to flow. • Metabolic • Neural
Left coronary flow during systole is depressed even though the pressure gradient is highest at that time. The effect is less dramatic in the right coronary because the compressive forces in the tissue are much lower in the right ventricle
A radial compressive stress exists in the ventricle that has zero pressure at the epicardium and increases to luminal pressure at the endocardium
Flow = Δ pressure / resistance Flow = (Arterial-Venous) / resistance Arterial pressure Pressure profile Extravascular pressure = 0 Venous pressure
Flow = Δ pressure / resistance Flow = (Arterial-ExVasc) / resistance Arterial pressure Pressure profile Extravascular pressure Venous pressure Vascular waterfall
During systole flow stops at the subendocardium but is hardly affected at the subepicardium. During diastole there is a reactive hyperemia in the subendocardium to make up for flow lost in systole. Autoregulation causes the reverse diastolic gradient.
Three Factors Control CBF • Mechanical • Metabolic: Autoregulation matches flow to metabolic need. • Neural
B C A Autoregulation makes flow independent of perfusion pressure. B is on the instantaneous line while C is on the steady-state line
If heart rate slowed, it would be shifted down. Flow Is Intimately Coupled to Myocardial O2 Consumption If heart rate were increased the steady-state line would be shifted up.
Energy requirements = internal + external Pressure External Work Internal Work Ventricular volume Increasing contractility increases oxygen demand
Reducing contractility with a beta blocker would shift the line down. Contractility Affects Coronary Blood Flow Increasing contractility by stimulating the sympathetic nerves would shift the line up.
hypoxia ATP adenosine + 3Pi Metabolites such as adenosine are released when flow does not meet the metabolic demand. These factors then dilate the coronary arteries to increase the flow. Robert Berne
Autoregulation compensates the loss due to mechanical factors so that flow across the wall is uniform despite the added mechanical impediment to flow in the deep layers
If coronary perfusion pressure is reduced due to narrowing flow to the subepicardium is maintained through dilation. However, vessels in the subendo-cardium have already expended their reserve.
The DPTI/TTI ratio is a rough supply demand index for the heart angina Gerald Buckberg & Julian Hoffman
III. Three Factors Control CBF • Mechanical • Metabolic • Neural: the coronary arteries have only limited neural control.
Increased contractility and heart rate causes net secondary dilation due to increased oxygen consumption (metabolic control wins over direct neural control of the coronary arteries vessels). Sympathetic stimulation Causes a weak Alpha - constriction that is only transient
A reduced coronary sinus PO2 indicates that the coronary flow is not as high as the heart would have liked. (some residual constriction) Eric Feigl
The parasympathetic stimulation has virtually no primary effects because few vagal fibers reach the ventricle (would have dilated the arterioles). A secondary vasoconstriction can be seen from autoregulation because reducing the heart rate reduces metabolic demand.
Coronary collaterals: (anastomoses between the coronary arterial branches) Collateral vessels maintain some tissue blood flow after complete occlusion of an arterial branch. This residual blood flow is nutritional and most non-reperfused infarcts are not transmural thanks to collateral flow.
Native collaterals can provide about 10-20% preocclusion flow in humans. That is not enough to prevent infarction. • Gradual occlusion over months as occurs with a developing atherosclerotic plaque causes collateral development. Some patients even have complete occlusion with few symptoms.
Collaterals occur at a level high above the arterioles (artery to artery). Thus they supply the entire occluded bed equally. Cells located close to the margins of an ischemic zone have no advantage
The borders between the fields perfused by adjacent coronary branches are very sharp. There is no tissue that receives a dual circulation. Michael V. Cohen
Three factors determine infarct size 1. Sizeof the ischemic zone 2. Level of collateral flow 3. Duration of ischemia
Therapeutic growth of collaterals with angiogenic factors such as VEGF have been tested but the results are not promising.
Three factors determine infarct size 1. Sizeof the ischemic zone 2. Level of collateral flow 3. Duration of ischemia
A wavefront of tissue death starts at the endocardium and progresses to epicardium over a 6hr period. Hearts can be made resistant to infarction with salvage-inducing drugs (still experimental) Robert Jennings
ischemic preconditioning, a 4th determinant of infarct size Shows that infarct size can be modified Preconditioned 40 min 50 40 30 % Infarction of the Ischemic Zone 20 10 0 Control Murry et al, Circulation 1986;74:1124-1136
The heart normally derives most of its energy from oxidative metabolism of lipids. Could simple loss of ATP be the determinant of life or death? Howard Morgan
ATP Glucose Glucose 6 phosphate hexokinase Cell death correlates well with loss of ATP in the cell. The cell needs ATP to phosphorylate Glucose for anerobic metabolism and to complex FFA with Acyl CoA.
This study showed that hearts that were protected against ischemia by preconditioning actually had lower ATP levels during ischemia but had less cell death than the controls. Clearly ATP is not the critical factor Kolocassides KG et al. J Mol Cell Cardiol. 1996 May;28(5):1045-57.
Osmotic swelling Hypothesis Cells are in osmotic equilibrium and cannot tolerate an osmotic imbalance. H2O Proteins The cell is full of osmotically active agents and is surrounded by ISF which is virtually protein-free 1 mM of an osmolyte exerts 19 mmHg pressure. Nucleotides Taurine
To keep the cell in equilibrium it pumps out sodium using it as the extracellular osmolyte H2O Proteins Nucleotides Taurine NA+ NA+
During ischemia ATP is broken down to AMP and two inorganic phosphates thus tripling the osmotic pull of the nucleotides. 5mM ATP 5mM AMP + 10mM Pi H2O Proteins Nucleotides Taurine NA+ NA+
Loss of ATP hinders pumping out the NA+. After 30 min of ischemia intercellular sodium will rise by 25 mM 25 mM Na+ 5mM ATP 5mM AMP + 10mM Pi H2O These two events alone increase the transmembrane pressure by: 35 x 19 or 665 mmHg Proteins Nucleotides Taurine NA+ NA+
During Reperfusion the ISF normalizes and water moves into the cell unimpeded with “explosive” swelling. H2O This type of cell death has been termed oncosis Proteins Nucleotides Taurine NA+ NA+
Blebs and vacuoles are seen. Mitochondria are swollen. The sarcolemma is lifted from the sarcomeres but retain the z-line attachments. 40 min of ischemia
The membrane is disrupted. Calcium has entered the cell and caused hypercontracture of the sarcomeres. cb = contraction bands 30 min of reperfusion
The free radical hypothesis Catalase SOD
A major source of free radical is xanthine oxidase. During ischemia adenosine reaches uM levels in the ISF In the 1980s Neil Granger working with Joe McCord here at USA showed that xanthine oxidase-derived radicals lead to cell death in the ischemic bowel of the cat. Joe McCord