Download
1 / 28
280 likes | 300 Views
Explore the intricate lifecycle of Lyme disease, symptoms, diagnosis, co-infections, associated lab findings, treatments, and variations in treatment approaches. Learn about early, disseminated, and late-stage manifestations, along with guidelines from IDSA and ILADS for managing this challenging condition.

E N D
The Lyme Enigma • Complexity and Controversy
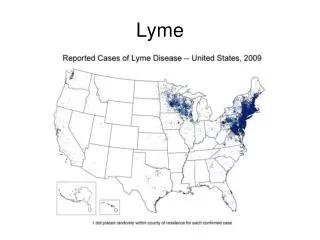
Lyme Life Cycle • Lyme disease is caused by a tick-borne spirochete, Borrelia burgdorferi. • Humans are an incidental host • The lifecycle of the spirochete is predominantly between mice, deer and the deer tick. In CA ixodes pacificus is the vector and in the east coast it is ixodes scapularis • The nymph deer tick is the most likely to transmit Lyme, and they are generally feeding in the spring and summer, adults feed in the fall
A closer look • Borrelia burgdorferi is found in NA. But also B miyamotoi • Borrelia garinii and afzelii are found in Europe. Or American patients returned from Europe. • Ticks are not the only way to get Lyme: sexual and placental transmission
Early signs and symptoms of Lyme • Erythema Migrans onset 7-14 days after bite • Sore throat, myalgias, arthralgias, fever, chills, and headache within days to 2 weeks after infection • If symptoms are severe and high fever is present consider co-infection with human granulocytic anaplasmosis(HGA) and Babesia. • Babesia microti/duncani in the East and babesia duncani in CA
Early disseminated Lyme • Arthralgias, • Neurologic symptoms, headaches, cranial neuropathy, diffuse or focal mononeuropathy multiplex, lymphocytic meningitis, plexopathy, • Radiculoneuropathy (Bannwarth syndrome) • Cardiac symptoms syncope, dyspnea, chest pain, palpitations, A-V block • Skin involvement-secondary erythema migrans, acrodermatitis chronicum atrophicans
Late Lyme disease • Occurs months to years after infection and often a period of latency • Joint and neurologic symptoms most common • Sub acute encephalopathies, axonal neuropathies and peripheral neuropathy • Bannwarth syndrome • Neuropsychiatric symptoms
Diagnosis • antibodies, • antigen, • PCR, • T-cell response, • culture
Direct testing • PCR • Lyme antigen • Coyle’s research
Antibodies • Initial lag time to seroconversion • Conversion of IgM to IgG • sensitivity of ELISA • sensitivity of WB • WB comparison • C6LPE • afzelii and garinii • Coyle’s research
T-cell response • aka iSpot
Lyme culture • fussy bug: • long incubation, preferred media, preferred surfaces
Associated Lab Findings • low CD57, low WBC • possibly low IgG3 or slightly elevated ANA • normal ESR, CRP • first-degree heart block
Co-infections • Babesia, Bartonella, Ehrlichia, Anaplasmosis...
Treatments • antibiotics, • herbs, • oxidative therapies, • silver
IDSA Treatment of early Lyme disease without significant neurological or cardiac symptoms • Doxycycline 200mg bid • Amoxicillin 500mg tid • Cefuroxime 500mg bid • All the above are given for 14-21 days
ILADS treatment of Erythema Migrans without other symptoms • Doxycycline 100mg qid or 200mg bid with food • Cefuroxime 1g bid • Amoxicillin 1g tid with probenicid 500mg tid if pregnant dose Amoxicillin q6h • Treat for 21 days • If pregnant treat for 6 weeks and test for Babesia, HGA, and Bartonella
IDSA treatment of Lyme carditis • Ceftriaxone 2gm qd for 10-28 days • Doxycycline 100-200mg po bid for 10-28 days • For AV block or myopericarditis use either of above regimes with appropriate inpatient monitoring. With resolution of heart block patient may be discharged home on po meds
ILADS Early disseminated Lyme • Milder symptoms present for less than one year with multiple Erythems Migrans lesions, constitutional symptoms, and lymphadenopathy, • Treat with oral therapy until no active disease for 4 weeks (4–6 months typical) using same antibiotic doses as outlined for Erythema Migrans • Pregnancy: As in Erythema Migrans, but duration as above. Treat throughout pregnancy, and do not breast feed.
IDSA treatment of late Lyme disease arthritis • Doxycycline 100mg bid • Amoxicillin 500mg tid • Cefuroxime 500mg bid • Treat for 28 days • If persistent or recurrent joint swelling retreat with another 28 days of above antibiotics or 2-4 weeks of IV ceftriaxone
IDSA late neurologic Lyme disease • This includes encephalopathy's and radiculopathies, Bannwarth syndrome • Treat with ceftriaxone 2 gm qd for 2-4 weeks • “Response to treatment is usually slow and may be incomplete” • “Re-treatment is not recommended unless relapse is shown by reliable objective measures”
ILADS Late Disseminated/ Chronic Lyme • Symptoms present greater than one year, more severely ill patients, and those with prior significant steroid therapy or any other cause of impaired immunity: • Treat adults and pregnant woman with 10 or more weeks of IV therapy , then oral or IM till asymptomatic for 6-8 weeksChildren: IV therapy for 6 or more weeks, then oral or IM follow up as above.
IDSA treatment of late Lyme disease arthritis • Doxycycline 100mg bid • Amoxicillin 500mg tid • Cefuroxime 500mg bid • Treat for 28 days • If persistent or recurrent joint swelling retreat with another 28 days of above antibiotics or 2-4 weeks of IV ceftriaxone
IDSA late neurologic Lyme disease • This includes encephalopathy's and radiculopathies, Bannwarth syndrome • Treat with ceftriaxone 2 gm qd for 2-4 weeks • “Response to treatment is usually slow and may be incomplete” • “Re-treatment is not recommended unless relapse is shown by reliable objective measures”
IDSAPost Lyme disease syndrome proposed definition • Onset of the following symptoms within 6 months of a documented case of Lyme that has been treated by IDSA guidelines • Fatigue • Widespread musculoskeletal pain • Complaints of cognitive difficulties • Exclusion of any diagnosable disease
Why antibiotic treatments don’t work • three forms of lyme (spirochete, L-form, cyst) • biofilm • tissue sequestration • patient’s intolerance to treatment: toxicity, gastritis, mycosis, mitochondrial fatigue • co-infections • evolution of bacteria, i.e. resistance • targeted vs comprehensive treatment strategy 25
Why treatments don’t work • Immune evasion • Using proteins that look like ours (ID badges), avoid recognition and therefore destruction by complement pathway. • Mutate surface proteins. Encysting. • Using proteins that look like ours (feeding misinformation), activate the immune system non-productively
Immune Evasion • Modulation of it’s surface antigens, OspA and OspC • Evades complement pathway: OspC, CD59-like complement inhibiting protein • OspA potent neutrophil stimulator and inducer of IL-1b, TNF-a, and IL-6 • Induces IL-10 initially to downregulate immune response • Delayed conversion of IgM to IgG
Comprehensive Support • anti-inflammatory: diet, herbs, proteolytic enzymes • lymphatics: walking, skin brushing, massage • gastro-intestinal: probiotics, regularity • liver support: phase I and II • brain/nerves: B12, herbals • methylation, glutathione • emotional/spiritual