Download
1 / 34
340 likes | 365 Views
Explore best practices in managing the transition to adulthood for adolescents living with HIV, focusing on challenges, clinical cases, and the importance of youth-friendly health services. Discover strategies for successful care and treatment, including adolescent interventions and the need for specialized approaches. Gain insights into the HIV prevalence among adolescents and the evolving health system responses.

E N D
Best practices in managing transition to Adulthood for Adolescents living with HIV Experiences from eThekwini AWACC Elangeni Hotel, Durban 19 Nov 2015
Adolescence – the inevitable maze Alexandra Nechita
Our future… their future view. • Client lists 3 life goals (High VL) versus her sister’s life goals (LDL) - • “To help my family “ • “ To be with my family “ • “To be good in my schoolwork “ • Versus • “ Finish my studies( all of it)” • “ Doctor ( go to medical school )” • “ Actress ( act in horror movies )”
Growing up… society in transition External Internal
Outline • Part 1: Background – Why should I pay attention? • Part 2: Towards Adolescent and Youth friendly health services • Part 3: Clinical Cases – any quick fixes? • Part 4: Transition to Adulthood
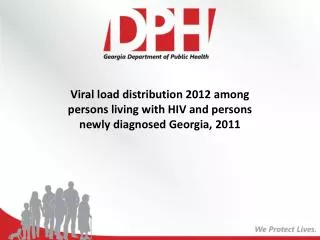
HIV Prevalence by Age, Gender in South Africa (2012) Adolescent girls 15-19 are up to 8 times, while young women 20-24 are more than 3 times, more likely to be infected with HIV than their male peers.
Summary of epidemiology • Adolescents (aged 10-19) accounted for an estimated 25% of all HIV infections in South Africa • Centre of the epidemic in terms of infection rates (incidence up to 2.54 in young females), vulnerability (teenage pregnancy, risk behaviour, gender-based violence, inequalities and impact) • Increasing numbers of perinatally infected children are now reaching adolescence • Increasing access to HCT and ART
What about health system response? I am a real ADULT Not a child, not yet an…
Focus on the cascade… 90% of all people living with HIV will know their HIV status 90% of all people diagnosed with HIV will receive sustained antiretroviral therapy. 90% of all people receiving antiretroviral therapy will have durable suppression.
Part 1: Take home messagesBackground – Why should I pay attention? • This is a sizable population • A growing population at the heart of the HIV epidemic • It is a unique population - labile physiological growth phase – pivotal to future productivity and function • Adolescents embody every community's hopes for the future. Adolescence is a time of vibrancy, self-discovery and rapid change or growth • Not children and not yet adults • Health care providers and health system ill equipped to deliver clinical and psychological services to adolescents living with HIV infection
Questions and Answers Q. The adolescent package of HIV care closely resembles the package of HIV care for adults; however, the way services are delivered can impact their success among adolescents. • True • False
Adolescent Youth Friendly Services • Advocacy • MDT • Baseline • Training • Planning • Quality cycle • There are successful models of adolescent HIV care and treatment services. These models can be adapted and scaled-up nationally. • Health workers need the knowledge and skills to meet the specific needs of adolescent clients.
Characteristics of Youth-Friendly Services Source: Senderowitz, J., Solter, C., & Hainsworth, G. (2004). Comprehensive reproductive health and family planning training curriculum. 16: Reproductive health services for adolescents. Watertown, MA: Pathfinder International.
Effective adolescent interventions • Motivational interviewing • Cognitive Behavioural • Incentives • Technology *The Adolescent Medicine Network For HIV/AIDS prevention *The Lancet 2014 – Rashida Ferrand et al
Challenges • Health education, human rights • Testing during adolescence • Condom use and prevention • Access to treatment and care • Substance use • Isolation / psychological transition and social complexity • Have unique psychological, cognitive, physiological and neurological developmental issues • Risk-taking behaviour • Adherence, Amplified barriers • Goals include wellness, economic participation and social cohesion
Part 2: Take home messagesTowards Adolescent and Youth friendly health services • Regardless of how long they have been infected or how they acquired HIV, the package of care for all ALHIV is very similar. • The approach for all adolescents should be family-centered and developmentally appropriate. • While the components of the adolescent package of HIV care closely resemble those of the adult package, the way these components are delivered has an important impact on their uptake and success among adolescents.
A case of disclosure • 13 year old male • Started ARVs at CHC: 01/05/2005: D4t/3TC/EFV • Transferred to Regional: Nov 2011 • 28/02/2012 ABC/3TC/EFV – Lipodystrophy on Stavudine • Partial disclosure: 5/12/2014 revisited disclosure counselling 4/2/15 + 6/8/15. Reluctance by caregiver is not allowing completion of full disclosure but counselling and support is on-going.
A case of recurrent defaulting • 12 year old male • ART started: 6.07.2009: D4T/3TC/EFV • PTB on abn CXR / TB symptoms/ smear negative: 10.05.2010 • Defaulted ART for 4 months. Returned to care on 30.05.2011. Restarted TB meds for Disseminated TB • Restarted ART at Regional: Aug 2011: ABC/3TC/EFV • Transfer ART care to CHC 20.10.2011. • Defaulted again for 7 months: May – Dec 2014 • Returned back to care: 5.12.2014 • Reinitiated ART: 18.12.2014: ABC/3TC/EFV • COR to second line: 27.08.2015: AZT/3TC/LPVr • Completed full disclosure: 27.08.2015 .
A case of peer support group intervention • 18 year old male • ART started: 11.03.2009: D4t/3TC/EFV • Current ART: second line: AZT/3TC/LPVr • ? Exact date of initiation: old file lost • Full disclosure: 19.03.2014
Part 3: Take home messagesClinical cases • Managing adolescent cases is difficult • One size does not fit all • There are no quick fixes • A multidisciplinary approach is required • A plan is required • Follow-up by the same team keeps things going forward
Questions and Answers (Continued) Q. Disclosure to a child or adolescent is a one-time event for which the caregiver must be well-prepared. • True • False
Disclosure Process SA HIV Disclosure Guidelines for Children and Adolescents 2014
Disclosure: Key Points • Disclosure is an ongoing process, not a one-time event. • Disclosure can help young clients access prevention, care, treatment, and support. It can also improve adherence, reduce stigma and discrimination, and slow the spread of HIV by helping people protect themselves and their partners. • Disclosure can result in health benefits for the child/ adolescent and caregiver. • Health workers and caregivers may face barriers to disclosure, such as not knowing where to start or feeling concerned about harming the child/adolescent.
Questions and Answers Q. Adherence preparation and ART initiation can usually be completed in 1 visit. • True • False
Risk to treatment failure (ROTF): Purpose • Provide structured adherence support for patients with HIGH viral loads • Provide standardised adherence messages to common adherence barriers • Prolong the duration of Viral Load suppression on 1st line and 2nd line ART • Ensure timely and successful regimen changes • Limit the need for 3rd line ART
Role of MDT in ROTF Enhanced Counselling • Administrative staff – Get and review results, can flag the patient’s file, enter results/data on Tier.net • Counsellor – Offer standardised adherence messages and motivate patient. Facilitate support groups • Nurse/ Doctor – Standardised adherence support, clinical support, viral load monitoring and correct regimen choice. • Social Worker- Address psychosocial Issues
Summary of steps on the ROTF adherence worksheet Adapted from MSF Khayelitsha Treatment Failure Model
Adolescent support groups • Teens only communicate with other teens • Peer Pressure • Peer Counsellors • All have similar anxieties fears questions • Eg Sexuality, prognosis, child bearing,disclosure ,preventing transmission,transitioning to adults • Logical to discuss these in a group • Run by responsible person that teens trust • Can be run by older teens themselves with adult supervision • Set programme of topics for discussion
Health Education and Related Topics That Can Be Incorporated into Support Group Meetings: • Positive living • Adherence • Disclosure • Sexual and reproductive health • Relationships and sexuality • Preventing new HIV infections and positive prevention • Preventing OIs • Coping with school • Finding work • Strategies to reduce gender- based violence • Dealing with stigma • Nutrition • Getting help for mental health problems • Dealing with dying and the death of a friend or family member • Managing disabilities
Transition from Pediatric to Adult Care • The goal of transition is to ensure the provision of uninterrupted, coordinated, developmentally- and age-appropriate, and comprehensive care before, during, and after the transition. • ALHIV may face challenges: • In their transition to adult care • In learning to independently manage their own care • These challenges affect ALHIV, their caregivers, and health workers in pediatric and adult clinics.
Key Considerations for the Transitionto Adult Care • All adolescents require support both within and outside of the clinic setting to take greater ownership over their health care, behavior, lives, and adherence. • The transition to adult care often occurs in parallel with an adolescent’s emotional and physical maturation. Effective transition must allow for the fact that adolescents are undergoing changes that impact much more than just their clinical care. • Health workers should: • Help ALHIV set and achieve goals for independence and self-management of care • Encourage ALHIV to develop as much independence as possible • Support caregivers to understand their changing role
Part 4: Take home messagesTransition towards adulthood • Communication – seek first to understand • Managing the process, communication within the health system • Facility ownership of transition service – know and monitor your own data and targets • Managing Disclosure • Risk of treatment failure • Adolescent Support Groups • Creating a future worth striving for