Download
1 / 49
530 likes | 764 Views
LEUCOCYTES. Presented by Prof. Dr Gehan Sheira Tanta University 2006-2007. LEUCOCYTES. The white blood cells may be divided into two broad groups, the phagocytes and the immunocytes. The phagocytes are the granulocytes ( neutrophils-eosinophils- basophils) together with the monocytes.

E N D
LEUCOCYTES Presented by Prof. Dr Gehan Sheira Tanta University 2006-2007
LEUCOCYTES • The white blood cells may be divided into two broad groups, the phagocytes and the immunocytes. • The phagocytes are the granulocytes ( neutrophils-eosinophils- basophils) together with the monocytes. • The lymphocytes (B and T) and plasma cells make up the immunocyte group. • Only mature phagocytes and lymphocytes are found in normal peripheral blood. Stab(band)neutrophils may occur in normal peripheral blood. • The role of phagocytes and immunocytes in protecting the body against infections is closely connected with tow soluble protein systems of the body,the immunoglobulins and the complement.
- In the bone marrow leucocytes differentiation and maturation occur:
Leucocytes are found in the peripheral blood as they migrate from bone marrow to the tissues. • The leucocytic number ( total and differential ) is remarkably constant with minor diurnal variation. 9 • Total LC 4-8 x 10 / L • Diff LC Neutrophils 40- 75 % • Lymphocytes 20- 35 % • Monocytes 2 - 8 % • Eosinophils 1 – 4 % • Basophils < 1 % . • Polymorphonuclear granulocytes ( neutrophils – basophils – eosinophils ) with cytoplasmic granules which stain either with acid eosin or alkaline ( basic ) reactions . Monocytes and lymphocytes are mononuclear ones .
-Control of granulopoiesis: Many growth factors ( GF ) are involved : - IL 1,3,5 for eosinophils - IL 6,11, GMCSF , GCSF and monocytes CSF ( MCSF ) . GFs stimulate proliferation , differentiation and function of the mature cells . Infections increase production of GFs from T- lymphocytes and stromal cells stimulated by IL 1, TNF and endotoxin .
-Clinical application of GFs : IV or SC administration of GFs(GMCSF and GCSF ) increases neutrophils , eosinophils and monocytes : • Severe neutropenia . • Severe infections as adjuvant to antimicrobial therapy . • Post chemotherapy , radiotherapy or BMT to decrease infections , usage of antibiotics and time in hospital . • Myelodysplasia to improve BM function . • AML to stimulate myeloid blast cells into cell cycle enhancing their sensitivity to chemotherapy .
Lymphocytes • Lymphocytes are the immunologically competent cells which assist the phagocytes in the defence of the body against infections and other foreign invasion . • Lymphoid organs : primary lymphoid organs in which lymphocytes develop are the bone marrow and the thymus , the secondary lymphoid organs in which specific immune responses are generated are the lymph nodes , spleen and lymphoid tissues of the alimentary tract and the respiratory tract .
-Lymphocytes orginate from stem cell in the bone marrow : • Some (75 % ) migrate to the thymus where they differentiate into mature T- cells during passage from cortex to medulla . • T- lymphocytes are divided into helper cells ( CD 4 ) and suppressor or cytotoxic cells ( CD 8 ) . • Others become B – lymphocytes . • And few become cytotoxic or Natural killer cells .
In BM B –lymphocytes > T-lymphocytes • In blood T-lymphocytes > B-lymphocytes • Both B and T lymphocytes respond to antigenic stimuli by transformation • -B-lymphocytes become plasma cells producing the immunoglobulins.Plasma cell is larger than B-lymphocyte with an eccentric round nucleus . • -T-lymphocytes mediate cellular immunity • The life span of lymphocytes may vary from few days to many years .
Lymphocytosis • Causes : 1-Infections : • acute :infectious mononucleosis , HIV ,herpes , mumps , hepatitis , cytomegalovirus . • chronic : TB , brucellosis , toxoplasmosis 2- ALL 3- CLL 4- Non Hodgkin lymphoma
Lymphopenia • Causes : 1-Severe BM failure with immune suppressive therapy 2-Immune deficiency syndromes primary or secondary ( AIDS ) .
Monocytes • These derive from CFC-GM in the BM. • They are charecterised by irregular shape nucleus in cloudy granular cytoplasm. • They are motile phagocytic cells migrate into the tissues where they develop into various types of macrophages ( tissues macrophages – Kupffer cells – oesteoclasts ).
-Functions of monocytes : • -remove debris and microorganisms by phagocytosis • -present antigenic material to T-lymphocytes. • -lysis of tumours ( tumour necrosis factor ) • -Tumour necrosis factor ( TNF) and IL 1 produced by monocytes are considered as mediators of acute phase response. • Life span of monocytes lasts for months.
Monocytosis -Causes : 1 -Chronic infections ( TB , typhoid and brucellosis ). 2 -Treatment with MCSF and GMCSF. 3 -Hodgkin disease. 4 -Myelodysplasia and CMML .
Basophils • -Poorly phagocytic cells • -Participate in hypersensitivity reaction as they possess receptors for the Fc portion of the Ig E on specific site on the cell membrane. • -Release of histamine occurs with degranulation of the cells. • -Basophils also contain heparin. • -Basophilic leucocytosis occurs in myeloproliferative disorders.
Eosinophils • -T-lymphocytes appear to exert some control on eosinophils production. • -They are also phagocytic but less than neutrophils. • -Participate in hypersensitivity reactions, associated with allergic reactions and ingest antigen antibody complexes. • -They have a role in the containment of parasitic infections. • -Their numbers are severely reduced by corticosteroid therapy.
Eosinophilic leucocytosis - Causes : 1-allergic and hypersensitivity diseases. 2-parasitic diseases. 3-certain skin diseases ( psoriasis……) 4-treatment with GMCSF 5-Hodgkin s disease. 6-hypereosinophilic syndrome 9 eosinophilic number is more than 1.5 x 10/L for more than 6 months with tissue damage for example heart valves , lung and skin.
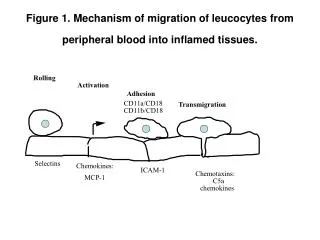
Neutrophils • Production of neutrophils takes place in the BM. • Mature neutrophils leave BM and circulate in the blood ( 8 hours ) then leave the circulation by adhering to capillary endothelium ( margination ) and migrate through the vessel wall into the tissues where they function. A considerable proportion of neutophils in blood is marginated. • -Stress factors ( infection – emotion – exercise ) may return these cells to circulation raising the leucocytic count .
-Life span of neutrophils is about 3- 4 days . • -Immature forms ( myelocytes ) are found in the blood when production of leucocytes is being stimulated (severe pyogenic infection ) . • More primitive forms ( myeloblasts ) appear in the blood indicating a serious disturbance of marrow function as in leukemia and invasion of BM by metastases . • -A particularly marked neutrophilia may be termed leukaemoid reaction and may be seen in life threatening infection , some cancers and severe haemolysis .
-It may be impossible to distinguish chronic myeloid leukaemia from a leukaemoid reaction on the blood count alone , but on the demonstration of a decreased neutrophil alkaline phosphatase score ( NAP : 20- 100 ) and the presence of Phladelphia chromosome on analysis of BM .
Function of neutrophils • -Neutrophils are phagocytic cells which ingest bacteria and fungi . They are attracted to bacteria by chemotaxis and phagocytosis is increased by opsonization stimulated by Igs and complement as phagocytic cells have Fc and C3b receptors . • -Engulfed bacteria are destroyed by neutrophils lysosomes and enzymes . • -Autodigestion is a potent stimulant to fresh neutrophils formation and pyrogens are released .
-Neutrophils also ingest uric acid crystals and may disintegrate liberating tissue damage substances causing local inflammation . • -Neutrophils can produce vitamin B12 binding protein ( transcobalamin 111 ) . So , the increased level of B12 vitamin in serum in CML .
Neutrophil leucocytosis -Causes : 1- Bacterial infection ( pyogenic ). 2- Inflammation and tissue necrosis . 3- Neoplasms . 4- Acute haemorrhage and haemolysis . 5- Metabolic disorders ( uremia – gout -acidosis ) . 6-Treatment with GFs . 7- Myeloproliferative disorders . 8- Corticosteroid therapy as it inhibits migration .
- With neutrophil leucocytosis : • Fever with release of leucocyte pyrogen • Shift to the left with increased stab forms • Increase of the NAP score .
Neutropenia • Neutropenia exists when the absolute neutrophil count falls below 1500/ul . Agranulocytosis occurs • with complete absence of neutrophils in the peripheral blood • The neutropenic patient is increasingly vulnerable to infection by gram +ve and gram –ve bacteria and by fungi . The risk of infection is related to the severity of neutropenia .
Causes of neutropenia • All the causes of pancytopenia and aplastic anaemia may cause neutropenia. Isolated neutropenia and agranulocytosis are often due to an • idiosyncratic reaction to drugs or exposure to a variety of chemicals . • -Infections : -Viral , e.g. hepatitis, HIV, glandular fever.-Bacterial , e.g. miliary TB, typhoid, brucellosis.
-Drugs induced : -Antibiotics : sulphonamides –chloramphenicol co-trimoxasole . -NSAIDs : phenylbutazone …. -Anticonvulsants : phenytoin …. -Antithyroids : carbimazol …. -Antidiabetics : chlorpromide …. -Antihypertensive : captopril …. - Antiarrhythmic : procainamide …. - Antimalarial : chloroquine … - Miscellaneous : gold, penicillamine ….
-Bone marrow infiltration or replacement, e.g.leukaemia , lymphoma, myeloma and carcinoma . • -Immune : autoimmune , SLE , Felty s syndrome • -Hypersplenism . • -Congenital neutropenia ,Kostmann s syndrome,is a AR disease presenting in the first year of life with life-threatening infections . • -Cyclic neutropenia , it is a rare syndrome with 3-4 week periodicity , severe but temporary .
Clinical picture • Severe neutropenia is particularly associated with infections of the mouth and throat .Painful and often intractable ulceration may occur at these sites .Septicaemia rapidly supervenes . Cellulitis and pneumonia are common . • With severe neutropenia , the usual signs of inflammatory response to infection may be absent . • Treatment : - Treatment of the cause ,drug discontinuation. - Combination of broad spectrum antibiotics . - Myeloid growth factors may be of help ( GCSF – GMCSF ) .
Immunoglobulins • These are heterogeneous group of proteins produced by plasma cells . They are divided into five subclasses or isotypes : Ig G , Ig A , Ig M , Ig E and Ig D . Ig G is the common contributes of the normal serum immunoglobulin ( about 80 % ) and is further subdivided into four subclasses : Ig G 1 , G 2, G 3 and G 4 . Ig A is the main Ig in secretions , it is subdivided into to types . Ig M has the largest molecular weight . Ig D and E are involved in delayed hypersensitivity reactions .
The Igs are all made up of the same basicstructure , consisting of two heavy chains which are called gamma in Ig G , alpha in Ig A , mu in Ig M , delta in Ig D and epsilon in Ig E , and two light chains ( Kappa or Lambda ) which are common to all five Igs . They can be broken into a constant Fc fragment and two highly variable Fab fragments .
The main role of Igs is defence against foreign organisms . They have a vital role in the pathogenesis of a number of haematological disorders : • - Secretion of a specific Ig from a monoclonal population of plasma cells occurs in macroglobulinaemia and most cases of multiple myeloma . • –Bence Jones protein found in the urine in some cases of multiple myeloma consists of a monoclonal secretion of light chains or light chain fragments . • – Igs may bind to blood cells in a variety of immune disorders and cause agglutination or destruction of cells .
Multiple Myeloma • It is a malignant disorder of plasma cells . Plasma cells are derived from B-lymphocytes by transformation after exposure to antigenic stimuli . Plasma cells manufacture Igs with only one type of light chain ( Kappa or Lambda ). • In myeloma and other malignant disorders of B-lymphocytes , all the malignant cells produce the same Ig which indicates that the tumour is derived originally from one cell cloning ( monoclonal ).
The monoclonal Ig is called a paraprotein and appears on serum electrophoresis as clear cut band . In myeloma , the paraprotein produced belongs to one of the five Igs and has one or other of the two light chains . • Bence Jones proteinuria appears in patients with multiple myeloma when only part of the Ig molecule is produced by the tumour cells, most commonly the light chains .
Pathology and clinical features • -Multiple myeloma is a neoplastic proliferation of plasma cells , more common in males with a peak incidence between 60 and 70 years . • - It is charecterised by replacement of the BM by the malignant cells leading to anemia and later to general BM failure. • -IL6 is a potent growth factor for myeloma by an autocrine mechanism. • -Osteoclastic stimulation with absorption of bone resulting in diffuse osteoporosis , bone pain , lytic lesions and pathological fractures .
-Hypercalcemia is common and appears to be mediated by osteoclast activating factor ( OAF ) and similar lymphokines ( IL1, TNF ) causing thirst , lethary , polyuria , anorexia , vomiting and constipation . • -Malignant plasma cells can form solitary tumour plasmacytoma either in tissue or bone causing spinal cord compression . • -Excessive production of the paraproteins may cause hyperviscosity syndrome ( mucosal bleeding , vertigo , headache , visual disturbances , stupor and coma ) .
-Light chain components of Igs may cause renal failure aggravated by hypercalcemia , or may be deposited in tissues as amyloid leading to amyloidosis renal damage . • -Myeloma patients are prone to recurrent infections due to failure of antibody production , neutropenia and the effects of chemotherapy . Respiratory infections especially with H.influenza and streptococcus pneumonia . • -Abrormal bleeding tendency as myeloma protein may interfere with platelet function and coagulation factors , thrombocytopenia occurs in advanced disease .
Diagnosis and investigations -Detection of paraprotein ( monmclonal Igs or light chains in serum or urine by serum protein or immune electropheresis.
-Infiltration of BM by abnormal plasma cells usually > 20 % . • -Osteoporosis and osteolytic bone lesions ( skull , spine , ribs and proximal long bones ). • -Hypercalcemia , high ESR , anaemia , neutropenia and thrombocytopenia in advanced disease . • -Serum urea and creatinine are raised in 20 % of cases . Serum B2-microglobulin is a useful indicator of prognosis . • -On occasion the abnormal protein in urine is cryoprecipitable .
-Treatment: • -At early stage of the disease , with no symptoms, no specific treatment only observe the patients. • -All patients must drink at least 3lit. fluid daily that may completely reserve renal impairment and help to manage hypercalcemia with IV 90 mg of bisphosphonates monthly . • -Melphalan ( 7mg/m2 for 4 days every 4-6 weeks ) in combination with prednisolone may be effective in bringing the disease under control .
-Recently , in patients less than 60 years , more intensive combination chemotherapy is used such as C-VAM protocol ( cyclophosphamide , vincristine , adriamycin and methylprednisolone. ) • -Following several cycles of treatment most patients proceed to autologous stem cell transplantation ( SCT ) . Most patients unfortunately are not young enough to undergo allogenic transplantation .
-Interferon alpha may prolong the plateau phase following chemotherapy or transplantation . Thalidomide is showing promise in relapsed disease . • -Radiotherapy is highly effective in treating local problems as severe bone pain or spinal cord compression .
Infectious Mononucleosis • It is an acute infectious disease due to Epstein-Barr virus. • The disease is charecterised by a lymphocytosis caused by clonal expansions of T-cells reacting against B- • lymphocytes infected with EBV. • It may occur at any age but usually occurs between 10 and 35 years. • The virus infects and replicates in B-lymphocytes and is shed in the throat. So, transmission is usually by oral contact possibly by saliva. • The incubation period is 7 to 15 days.
-Clinical features: • Toxic manifestations early in the disease, malaise, tiredness, headache, anorexia, myalgia and fever. • Lymphadenopathy, discrete, non suppurative slightly painful esp. along posterior cervical chain. • Splenomegaly in about 50% of cases and hepatomegaly in about 15%. • Sore throat with exudative tonsillitis is usually present. • Maculopapular or occasionally petechial rash especially if ampicillin has been given.
-Complications: • 1- Haemolytic anemia, thrombocytopenia. • 2- Hepatitis, jaundice, rupture spleen. • 3- Aseptic meningitis and CNS involvement. • 4- Chronic fatigue syndrome.
-Investigations: • Predominance of atypical lymphocytes in the peripheral blood( larger than normal, vacuolated foamy cytoplasm, dark chromatin in the nucleus). • Hetrophile agglutination test, high titres occur during the second and third weeks. Hetrophile antibodies against sheep red cells form the basis of the Paul-Bunnell test, and against horse red cells instead in the monospot test. • Specific antibody to the EBV nuclear antigen. • Autoimmune haemolytic anaemia, and thrombocytopenia are frequent
-Treatment: • Symptomatic: rest, aspirin, NSAIDs, warm saline throat irrigations. • 5 day course of corticosteroids, prednisolone 50 mg/day for 3 days with tapering may be of beneficial. • Antiviral drugs are not helpful although newer agents( famciclovir ) appear to have anti EBV properties. • Treatment of complications.