Download
1 / 81
810 likes | 984 Views
Hypersensitivity reactions are exaggerations of normal defence mechanisms. Il termine allergia è stato originariamente coniato da Clemens Von Pirquet come una “capacità alterata del corpo di reagire ad una sostanza estranea” . ALLERGIA:

E N D
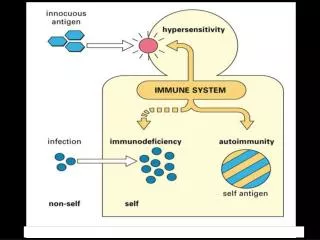
Hypersensitivity reactions are exaggerations of normal defence mechanisms
Il termine allergia è stato originariamente coniato da Clemens Von Pirquet come una “capacità alterata del corpo di reagire ad una sostanza estranea”
ALLERGIA: Malattia che deriva da una risposta del sistema immunitario ad un antigene innocuo L’allergia è un tipo di reazione del sistema immunitario classificata come ipersensibilità
Le reazioni di ipersensibilità sono classificate in quatto tipi da I a IV L’allergia è tipicamente l’ipersensibilità di tipo I
HYPERSENSITIVITY • TYPES I - IV I - IgE MEDIATED REACTION - • Binding of antigen to IgE on the surface of mast cells causes release of inflammatory mediators II - CYTOTOXIC REACTION - • Binding of antibody to cell surface leads to activation of complement and damage to host cell eg. blood cells (penicillin, methyldopa, quinidine)
HYPERSENSITIVITY III - IMMUNE COMPLEX REACTION (Arthus) - • Formation of complexes between antigen & antibody leads to tissue damage as a result of deposition in blood vessels (vasculitis) and activation of inflammatory pathways (serum sickness, farmers lung) IV - CELL MEDIATED REACTION (DTH) - • Activation of T cells around site of antigen leads to T cell cytotoxicity & activation of macrophages, causing tissue damage (contact sensitivity)
Allergy Hay fever, asthma, eczema. Atopy (Greek: ‘out of place’) 10-15% individuals clinically allergic 30% individuals show wheal and flare to skin tests for common allergens Asthma is the most common chronic disease of children in Western countries. Causes 2,000 deaths/year in UK
Epidemiology of Allergy • 50 Million Americans Affected • 10-22% Adults • 10-42% Children • Peak Incidence • Late Childhood • Early Adolescence
Genetics and Development of Allergies • Risk of developing allergies: • No parents have allergies- 10% risk • One parent has allergies- 40-50% risk • Both parents have allergies- 70-80% risk • Children with one allergic component (rhinitis, asthma, or eczema) have a 3-fold increased risk of developing others
Type I hypersensitivity IgE-mediated mast cell degranulation
Le IgE sono prodotte dalle Plasma cellule che si trovano nei linfonodi drenanti il sito di ingresso dell’antigene o localmente nel sito dove avviene la reazione allergica. Le IgE prodotte nei centri germinativi diversamente dagli altri anticorpi sono presenti a livello tissutale fortemente legate alla superficie delle mast cells attraverso i recettori FceRI
Sebbene non sia nota la ragione per cui alcuni Ag sono allergeni, sono emersi dei principi generali: La maggior parte degli allergeni sono proteine piccole altamente solubili portate da particelle essiccate come il polline o le feci degli acari
Allergens Proteins found in nature Trees Grasses Weeds Moles Dust mite feces Cockroaches Animal danders Enter the body by ingestion or inhalation, injection (insect venom, antibiotics) Al contatto con le mucose, ad esempio quelle del tratto respiratorio, gli allergeni solubili vengono eluiti dalle particelle e diffondono nelle mucose. Tipicamente sono presentati a dosi bassissime.
ALLERGENS • Antigens that initiate an IgE-mediated response • Contain B cell epitopes & T cell epitopes • Allergen requires processing by dendritic cells/macrophages • Presentation to T cells results in delineation of T-helper subsets into TH1 and TH2 types • TH2 responses lead towards IgE production Ag presentation at very low doses at the mucosal level favor the activation of Th2 responses. At the mucosal level the APCs are myeloid DC that present low antigen doses very efficiently, migrate to draining LN and activate Th2 responses
Immediate Hypersensitivity - Type I Hypersensitivity • Examples: Hay Fever type allergies, anaphylactic reactions • Reactions usually occur within minutes of exposure. • Develops when antigen combined with IgE attached to mast cells. Large amounts of mast cells in skin and mucous membranes of respiratory tract • IgE antibodies bind mast cells, basophils, cross link IgE receptors causing degranulation • Release of various mediators including histamine • Histamine causes hives, itching, stridor, laryngeal edema and wheezing • Leads to vascular leakage, especially venules • The arteriolar dilation leads to hypotension • Allergen immunotherapy can reduce specific IgE levels
EARLY PHASE RESPONSE MAST CELL • GM-CSF & IL-3 important for development • FceR1 present at high density • Cross-linking of FceR1 by allergen leads to activation of mast cell, resulting in :- • DEGRANULATION - Release of pre-formed mediators • SYNTHESIS OF LIPID MEDIATORS
PRE-FORMED MEDIATORS HISTAMINE • Stimulation of irritant nerve receptors • Smooth muscle contraction • Increase in vascular permeability KALLIKREIN • Activates bradykinin - similar actions to histamine TRYPTASE - role unclear
LIPID MEDIATORS • ARACHIDONIC ACID DERIVATIVES Phospholipase A2 Arachidonic acid 5-Lipoxygenase Cyclo-oxygenase Molti anti-infiammatori inibiscono il metabolismo dell’acido arachidonico. Aspirina: inibitore dell’enzima cicloossigenasi, blocca la produzione delle prostaglandine LEUKOTRIENES PROSTAGLANDINS LTA4 LTB4 LTC4 LTD4 LTE4 PROSTACYLINE THROMBOXANE A2 PROSTAGLANDINS D2, E2, F2a
Y Y Y Y Y Newly generated: leukotrienes, prostaglandins cytokines (IL4, IL13) Pre-formed chemicals: histamine, tryptase, heparin
Molti allergeni sono enzimi. Ad esempio un allergene noto è il Der p-1 che si trova nelle feci degli acari. E’ simile alla papaina, taglia l’occludina e si guadagna l’accesso alle APC subepiteliali. Non tutti gli allergeni sono enzimi alcuni sono inibitori di enzimi e molti sono a funzione ignota
IgE production: Induction of Th2 responses and CD40-CD40L interaction
IgE Serum concentration 100 ng/ml (IgG 15 mg/ml) Destroyed by heating at 56o for 30 minutes Half life: 2.5 days in serum, 12 weeks if bound to mast cells Elevated in: ·Certain parasitic diseases (e.g. schistosomiasis) ·Hyper-IgE syndrome ·Allergy Class switching to IgE promoted by IL-4 and IL-13, inhibited by g-interferon
Receptor Affinity Cellular distribution FceRI 1010 Mast cells, basophils, eosinophils, Langerhans cells, activated monocytes FceRII 107 B cells, T cells, platelets, macrophages, NK cells, follicular dendritic cells, eosinophils, epithelial cells FceR
Pollution Acts as a non-specific trigger factor Sulphur dioxide, nitrogen oxides, diesel exhaust particles (DEP) May increase mucosal permeability and thereby enhance antigen entry
Allergy Incidence DEP 2000 1960 Year
Seasonal vs Perennial Allergic Rhinitis • Seasonal - Symptoms recur each year during the same season • Antigens include: • tree pollen • grass pollen • weed pollen • molds • Perennial - Symptoms are persistent year-round resulting from constant challenge • Antigens include: • dust • animal dander • molds • cockroach
Early phase: Cross-linking of FceRI by allergen (immediate reaction starting within seconds) Late phase response: Caused by the release of leukotrienes chemokines and cytokines from mast cells. These products recruit other leukocytes including eosinophils, Th2 (this phase can easily convert into a chronic inflammatory response if the Ag persists and stimulate Th2 cells which recruit eosinophils and induce further IgE production, chronic asthma)
LATE-PHASE RESPONSE - 1 BASOPHILS • Similar properties to mast cells over longer time scale EOSINOPHILS • GRANULES contain cytotoxic proteins (ECP, EDN, MBP, EPO) • In tissues, RELEASE CONTENTS OF GRANULES - major source of tissue damage in allergic response T CELLS • CYTOKINE-DRIVEN ACTIVITY is the major source of PATHOGENESIS in allergic responses
Eosinophils • Increase during allergic response • Release enzymes which degrade histamine and other mediators of inflammation • Protects the body from some protozoal and helminth infections
Local effects: The effects of allergen reexposure are limited to the site at which mast cells degranulation occurs
Allergen inhalation Allergic Asthma Allergen-induced activation of submucosal mast cells in the lower airway Early/late phase response involved early: bronchial constriction and secretion of fluid and mucus chronic: continued presence of increased number of Th2 cells, eosinophils, neutrophils and other leukocytes
Allergen inhalation RHINITIS Allergic/non-allergic Allergic: perennial or seasonal type Blocked nose, often with eye symptoms Major aero-allergens include House dust mite, pollens Early/late phase responses are involved ALLERGIC CONJUNCTIVITIS
Skin allergy: urticaria, chronic eczema Early/late responses are involved Local injection of small amounts of allergen (stinging insect) Localized allergic reaction: local mast cells activation, local increased of vascular permeability (fluid extravasation and swelling) 8 hours later: more spread and sustained edematous response urticaria
Local effects or more general effects Food Allergies
FOOD ALLERGY MAJOR FOOD ALLERGENS • Water soluble glycoproteins 10 -60 kd • Heat, acid & protease stable • COW’S MILK • CHICKEN EGG • LEGUMES - PEANUT; SOYBEAN; TREE NUTS • FISH • CRUSTACEANS / MOLLUSCS • CEREAL GRAINS
FOOD ALLERGY - CLINICAL GASTROINTESTINAL ANAPHYLAXIS - • Within 2 hours of ingestion • Nausea , pain , cramps , vomiting , diarrhoea ALLERGIC EOSINOPHILIC GASTROENTERITIS - • Nausea & vomiting; diarrhoea , steatorrhoea • Peripheral eosinophilia in 50% of patients • Elevated serum IgE with positive RASTs
FOOD ALLERGY - CLINICAL RESPIRATORY • Upper and lower respiratory tract symptoms • Food allergens can provoke airway hyper-reactivity • Studies suggest 35 - 40% of children assessed for food allergy develop respiratory symptoms • 2 - 10% of asthmatic children have symptoms induced by food CUTANEOUS • Acute urticaria / angioedema said to be common • ‘Cause - and - effect’ usually obvious to patient • Eggs , milk , peanuts , other nuts in children - >90% of reactions
Systemic reactions Allergen introduced in the bloodstream or adsorbed from the gut Systemic anaphylaxis Disseminated mast cells activation General increase in vascular permeability: loss of blood pressure airways constrict-respiratory difficulties swelling in the epiglottis (suffocation) anaphylactic shock can occur: Drug administered to people with high specific IgE levels Insect venom Some food