Download
1 / 22
410 likes | 3.19k Views
PROTEIN ENERGY MALNUTRITION. Fatemeh beiranvand # 616 26/05/2014. Definition. protein–calorie malnutrition

E N D
PROTEIN ENERGY MALNUTRITION Fatemeh beiranvand # 616 26/05/2014
Definition protein–calorie malnutrition WHO "the cellular imbalance between the supply of nutrients and energy and the body's demand for them to ensure growth, maintenance, and specific functions." The term protein-energy malnutrition (PEM) applies to a group of related disorders that include marasmus, kwashiorkor, and intermediate states of marasmus-kwashiorkor. Causes : primary : due to dietary deficiency Secondary : due to a serious illness like tuberculosis, cancer or inability of the body to absorb nutrients for e.g. in bowel disease like ulcerative colitis, metabolic syndromes and long standing gastro-enteritis.
Dual-energy X-ray absorptiometry • also called Bone density scanning, used to measure bone loss. • DXA is today's established standard for measuring bone mineral density (BMD) • . also be used to measure total body composition and fat content • DXA is most often performed on the lower spine and hips. In children and some adults, the whole body is sometimes scanned.
Types: include: - marasmus:The term marasmus is derived from the Greek word marasmos, which means withering or wasting. • Kwashiorkor:The term kwashiorkor is taken from the Ga language of Ghana and means "the sickness of the weaning. - intermediate states of marasmus-kwashiorkor: This includes symptoms of both Marasmus and Kwashiorkar and represents the gravest form of PEM.
kwashiorkor • due to inadequate protein in the diet despite an adequate caloric intake • It is most common in areas of drought and famine • Children are affected more frequently than adults. • It typically starts after the child has been weaned and breast milk has been replaced with a diet low in protein, • although it can occur in infants if the mother is protein-deprived. • most prevalent in overpopulated areas of the world in underdeveloped and developing countries, particularly in sections of Africa, Central and South America, and South Asia. • Kwashiorkor is very rare in the United States, but does occur and is usually a sign of child abuse and neglect
Pathogenesis • Intake of CHOs is greater than the intake of protein. • -Total caloric intake is normal; however, it primarily consists of CHOs. • Visceral protein is predominantly decreased, whereas somatic protein is relatively unchanged. • Somatic protein is relatively unchanged, because CHOs are protein sparing.. • Visceral protein is decreased because the liver is unable to synthesize proteins (e.g., albumin and other proteins).
Clinical findings of kwashiorkor --Pitting edema and ascites ↓plasma oncotic pressure Caused by hypoalbuminemia leading to a loss of plasma oncotic pressure --Massive hepatomegaly Caused by a fatty liver is due to: Decreased synthesis of apolipoprotein Increased synthesis of VLDL --Diarrhea Due to mucosal atrophy in the small intestine with loss of the villi . Loss of disaccharidases problems with cellular immunity predispose patients to parasitic infections in the bowel.
others -Anemia 1)RBC precursors in bone are decreased, leading to anemia. (2)Multiple vitamin deficiencies are usually present, leading to anemia. --Cutaneous changes - Alternating zones of hyperpigmentation and hypopigmentation Increased risk for infections -Hair changes also occur with loss of color, leading to alternating bands of dark hair and light hair --Growth retardation Due to the lack of essential nutrients in the diet --Psychological disturbances Patients are usually apathetic, listless, and anorexic Increased risk for infections Cell-mediated immunity (CMI; T cells) is compromised, predisposing patients to parasitic infections.
Exams and Tests The physical examination may show an enlarged liver (hepatomegaly) and general swelling. Tests may include: Arterial blood gas BUN Complete blood count (CBC) Creatinine clearance Serum creatinine Serum potassium Total protein levels Urinalysis
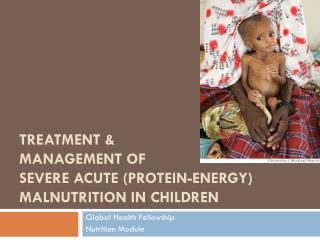
Marasmus – Chronic PEM • Common in Infancy, 6 to 18 months of age • Diet inadequate to meet needs for calories, protein, essential FA….watery cereal is primary food • Small for their age, < 60% weight-for-age, develop slowly • No edema or fatty liver
Pathogenesis a.Total calorie deprivation with a dietary deficiency of both protein and CHOs b. Decrease in somatic protein (muscle protein) - Extreme muscle wasting is common in marasmus
Clinical findings a.Extreme muscle wasting (“broomstick extremities”) (1)Due to the breakdown of muscle protein for energy (2)Loss of subcutaneous fat -Due to a decrease in leptin stores in the adipose, which stimulates the hypothalamic-pituitary axis to release cortisol, a lipolytic agent b.Growth retardation, anemia, defects in cellular immunity similar to kwashiorkor
Laboratory tests • Blood glucose • Examination of blood smears by microscopy or direct detection test • Hemoglobin • Urine examination and culture, Multistix • Stool examination by microscopy: • Albumin • HIV test • Electrolytes
Secondary PEM • Common in elderly ,choronicalcoholics,beddriddenpts • -Present in 30% to 50% of elderly individuals in hospitals or nursing home • --Factors responsible for reduced intake include: • Decrease senses of taste and smell • Suppressed appetite bcz of illnesses and medications • Depression • Advanced age
Clinical findings • -Depletion in subcutaneous fat and skeletal muscle similar to marasmus • -Ankle or sacral edema similar to kwashiorkor • -Increase risk for infection , or death after surgery
Treatment • Marasmus : • A nutritious, well-balanced diet with lots of fresh fruits and vegetables, grains, and protein will reduce the risk of malnutrition and any related marasmus • Kwashiorkor: • depends upon its severity. Fluid and electrolyte imbalances may need to be corrected with intravenous fluids, and infections may require treatment with Antibiotics
refrence • http://emedicine.medscape.com/article/1104623-clinical • http://kwashiorkor.eu/the-tale-of-two-diseases-the-difference-between-kwashiorkor-and-marasmus.php • http://emedicine.medscape.com/article/984496-workup • http://www.nytimes.com/health/guides/disease/kwashiorkor/overview.html • http://en.wikipedia.org/wiki/Protein%E2%80%93energy_malnutrition • Robbins Basic Pathology 8th edition • Rapid review pathology goljian