Download

1 / 14
140 likes | 159 Views
This interesting case report discusses a 25-year-old male with a 3-4 cm lump near the left testicle. The differential diagnosis includes epididymal cyst and solid paratesticular lesions. Surgical biopsy reveals splenogonadal fusion, a rare condition. This case emphasizes the importance of considering congenital anomalies and avoiding unnecessary orchidectomy.

E N D
A case that left us wondering... Dr Matthew Seager & Dr Miles Walkden BSGAR-BSUR Interesting Cases 2019 matthew.seager1@nhs.net
Clinical information • 25 male • 2 week referral by GP due to “3-4 cm” lump superior to the left testicle • Felt to be epididymal cyst, but could be testicular in origin O/E
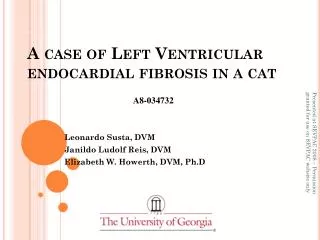
* Longitudinal section ultrasound image - left paratesticular region. * - epididymis thought to be separate.
Longitudinal section ultrasound image - left paratesticular region with colour Doppler
Transverse section ultrasound image – left paratesticular region with colour Doppler
Differential diagnosis ✗ - not cystic • Epididymal cyst Solid paratesticular lesions: • Adenomatoid tumour • Spermatic cord lipoma • Leiomyoma • Haemangioma • Sarcoma MDT decision: given vascularity -> surgical biopsy +/- excision ? - usually epididymal - tail ? -atypical appearance ? -not typically so vascular ? - extremely rare, but is vascular ? - long history of lump
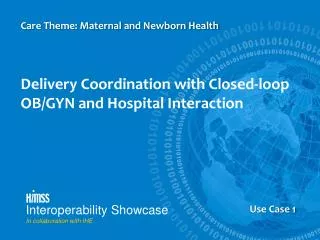
Final diagnosis • Lesion separate from epididymis at surgery • Closely associated with testicular vessels so not removed • 3 x biopsies obtained: • Ectopic splenic tissue • Given the location - final diagnosis of splenogonadal fusion
White pulp Red pulp
Discussion Splenogonadal fusion: • M:F 15:1, nearly all left • Close proximity of developing gonad and spleen in embryonic weeks 5-8 • Continuous or discontinuous • Continuous variety – 1/3 congenital abnormalities e.g. cryptorchidism, limb defects • Fusion with mesonephric derivatives rarely
Discussion • Presentation • 40% scrotal swelling • 20% inguinal hernia • 18% autopsy diagnosis • 15% cryptorchidism • 7% other • Imaging • Slight reduced reflectivity relative to testis • May be difficult to separate from testis – DD for testicular Ca • Central vascular pattern branching to periphery c.f. disorganised malignant • Difficult to pre-operatively suspect but 99mTc sulphur colloid diagnostic Varma et al. Marko et al.
Discussion Longitudinal section ultrasound image
Discussion • Management • Avoid unnecessary orchidectomy! • No evidence increased malignancy ✗
Key learning points • Rare condition • Consider splenogonadal fusion with a paratesticular mass and congenital anomalies • Awareness may allow appropriate pre-operative workup to avoid orchidectomy • Important to be aware of more common causes for solid paratesticular lesions
References • Putschar WGJ, Manion WC. Splenic-gonadal fusion. Am J Pathol. 1956;32: 15–33. • Carragher AM. One hundred years of splenogonadal fusion. Urology. 1990;35: 471–75. • Varma et al. Sonographic and CT features of splenogonadal fusion. PediatrRadiol. 2007;37(9): 916-9. • Marko et al. Testicular seminoma and its mimics. Radiographics. 2017;37(4): 1085-98. • Stewart VR, et al. Splenogonadal fusion. B-mode and color Doppler sonographic appearances. J Ultrasound Med. 2004;23: 1087-90.