Download
1 / 32
550 likes | 1.32k Views
Transcranial Magnetic Stimulation. Faten Alzaben PGY5 RESIDENT. What is it?. TMS is a non-invasive method of brain stimulation in which magnetic fields are used to induce electric currents in the cerebral cortex, thereby depolarizing neurons. Early Attempts!. Modern Application.

E N D
TranscranialMagnetic Stimulation Faten Alzaben PGY5 RESIDENT
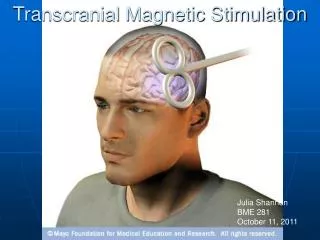
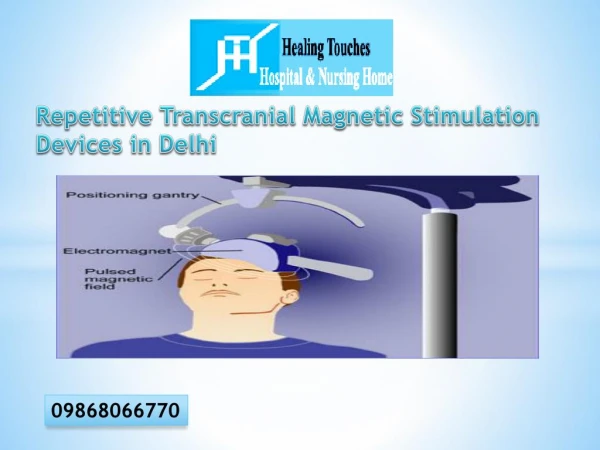
What is it? • TMS is a non-invasive method of brain stimulation in which magnetic fields are used to induce electric currents in the cerebral cortex, thereby depolarizing neurons.
History • the idea of using TMS goes back to the early 1900s. • 1985 tony barker and colleagues . • 1984 David Cohen, 1988 Shoogo Ueno : the idea and realization of the figure-of-eight coil .
Mechanism of action of TMS • Electrical energy is converted to magnetic fields ,which are then converted back into electrical currents in the brain. • TMS is sometimes called”electrodeless electrical stimulation”
Applications of TMS • A research tool to study aspects of the human brain physiology • Therapeutic application: • Neurological disorders • Psychiatric disorders
TMS as a research tool • A research tool to study aspects of the human brain physiology including motor function,vision,language and the pathophysiology of brain disorders • TMS can excite or inhibit the brain allowing functional mapping of cortical regions and creation of transient functional lesions.
Examples: • rTMS over the occipital lobe impaired detection of visual stimuli • rTMS delivered to discrete areas in the language-dominant hemisphere can disrupt speech.
Movement disorders: • Therapeutic applications of TMS in movement disorders are preliminary. • Fast rTMS of the motor cortex has been reported to improve performance on several motor measures in Parkinson disease. • a recent meta-analysis included 12 studies and concludes that the overall literature does show a positive effect of r TMS on Parkinson motor function. • Slow rTMS has been reported to improve dystonia. George, linsbey ,and sackiem Fregni et al. 2005
Neuro-rehabilitation • TMS to evaluate the functional properties of the motor cortex after lesions like stroke is of special interest in the field of neurorehabilitation. • Brain stimulation have been proposed to enhance motor function when combined with conventional neurorehabilitative interventions after stroke
Chronic Pain (rTMS) of the cortex induces analgesic effects in focalchronic pain syndromes.
Mood Disorders • Several studies demonstrated that repetitive transcranial magnetic stimulation (rTMS) is an efficacious treatment for treatment-resistant major depression. • its efficacy has often been shown to be modest, compared with sham stimulation.
Mechanisms of rTMS-Induced AntidepressantResponse • evidence suggests that MDD is most commonly associated with hypoexcitability over the left prefrontal cortex and hyperexcitability over the right prefrontal cortex
Evidence in support left prefrontal hypoexcitablity in depression: • Brain injury: • patients with left-sided strokes (hypoexcitability) experience depression • Patients with right-sided strokes experience manic symptoms • Imaging studies demonstrated that MDD may involve lower activity in the left DPLFC and higher activity in the right DPLFC.
rTMS treatment in MDD has often been shown to be associated with a normalization of hypoexcitability over the left prefrontal cortex and normalization of hyperexcitability over the right hemisphere.
Studies have demonstrated that when 10 Hz rTMS is applied to the right DLPFC , dysphoric symptoms occur.
Review of Studies of rTMS in Depression • Studies in the review were summarized into 5 broad categories: • 1- first-generation studies that have evaluated the efficacy of 10 rTMS sessions (that is, 2 weeks) for TRD. • 2-second-generation studies that have evaluated the efficacy of rTMS for more than 10 rTMS sessions. • 3-third-generation studies that evaluate the efficacy of rTMS using several novel treatment approaches (for example, bilateral rTMS). • 4- metaanalytic studies of rTMS for TRD. • 5-future studies proposing novel methods to optimize the efficacy of rTMS for TRD. The Canadian Journal of Psychiatry, Vol 53, No 9, September 2008
First-Generation Studies • rTMS studies applied at high frequencies (10 to 20 Hz) over the left prefrontal cortex have demonstrated efficacy in the treatment of depression. • Other studies also demonstrated right low-frequency rTMS to be useful in depression. • Other first-generation studies were equivocal or showed lack of efficacy. • Other studies have also reported negligible results.
Explanations : 1- most patients included in these studies were treatment resistant. 2- stimulation parameters including frequency, intensity, and duration vary from study to study. 3- concomitant use of medications . 4- no consistent method for precisely localizing the prefrontal cortex.
Second-Generation Studies • 20 or more treatments. • The results demonstrate that both HFL- and LFR-rTMS have substantial therapeutic efficacy.
Third-Generation Studies • bilateral rTMS. • The studies showed no difference between the groups. • Limitations of these studies: • First, bilateral rTMS was not compared with unilateraland sham rTMS in a sufficiently large sample of subject. • none of the studies were conducted for longer than 10 days . • none used more than 300 LFR-rTMS pulses.
Metaanalyses of rTMS in MDD • There have been at least 8 meta -analyses evaluating the anti-depressant effects of left DLPFC rTMS. All but one have shown greater antidepressant effects at 2 weeks of HFL-rTMS, compared with sham.
Limitations of Current rTMS Trials in MDD Factors underlie the relative modest therapeutic efficacy of rTMS studies conducted in MDD: 1- most of these studies involved left-sided treatment alone to the DLPFC. 2- suboptimal methods were used to target the DLPFC . 3-treatment durations were typically short (that is, 2 to 4 weeks). 4- stimulation intensity might have been insufficient by not taking into consideration coil-to-cortex distance
Anxiety Disorders • obsessive-compulsive disorder • posttraumatic stress disorder • panic disorder
Schizophrenia • reduced auditory hallucinations • reduced anxiety
Difference Between TMS and ECT • TMS: • does not require general anaesthesia • easy to administer in alert and wake subjects under medical supervision • no cognitive deficits reported at this point. • Does not involve induction of seizures
Adverse Effects of rTMS • Risk of inducing seizures (in patients with a hx or family hx of seizures).current safety protocols adjust the amount of stimulation in relation to the motor threshold of the individual. • Muscle tension headache . • Short term changes in hearing threshold related to the noise generated. • Cognitive changes only during stimulation