Download
1 / 25
460 likes | 1.2k Views
DIPHTHERIA. (BULL NECK). Diphtheria is an acute, toxin-mediated disease caused by Corynebacterium diphtheriae . The name of the disease is derived from the Greek diphthera , meaning leather hide.

E N D
DIPHTHERIA (BULL NECK) DR (MRS) M.B. FETUGA
Diphtheria is an acute, toxin-mediated disease caused by Corynebacterium diphtheriae. • The name of the disease is derived from the Greek diphthera, meaning leather hide. • Usually a disease of under-five children although non-immune young adults may also be affected. • No sex predilection is known. DR (MRS) M.B. FETUGA
BACTERIOLOGY • C. diphtheriae is an aerobic gram-positive bacillus, non-motile, non-spore forming. • There are three biotypes of C. diphtheriae — gravis, intermedius, and mitis. The most severe disease is associated with the gravis biotype, but any strain may produce toxin. • C. mitis-main type in Africa, appears to cause < severe disease DR (MRS) M.B. FETUGA
BACTERIOLOGY • Toxin production (toxigenicity) occurs only when the bacillus is itself infected (lysogenized) by a specific virus (bacteriophage) carrying the genetic information for the toxin (tox gene). • Only toxigenic strains can cause severe disease. • If isolated, the organism must be distinguished in the laboratory from other Corynebacterium species that normally inhabit the nasopharynx and skin (e.g., diphtheroids). DR (MRS) M.B. FETUGA
TRANSMISSION • Human carriers are the reservoir for C. diphtheriae, and are usually asymptomatic. • Transmission is most often person-to-person spread from the respiratory tract. • Rarely, transmission may occur from skin lesions or articles soiled with discharges from lesions of infected persons (fomites). DR (MRS) M.B. FETUGA
TRANSMISSION • Transmission may occur as long as virulent bacilli are present in discharges and lesions. • Schick Test is used to identify patients at risk of diphtheria. The toxin is injected intra-dermally. Subjects without previous exposure to the toxins lack the natural anti-toxins and they show a reaction. A positive test denotes susceptibility. DR (MRS) M.B. FETUGA
PATHOGENESIS • The organism produces a toxin that inhibits cellular protein synthesis and is responsible for local tissue destruction and membrane formation. • The toxin produced at the site of the membrane is absorbed into the bloodstream and distributed to the tissues of the body. • The toxin is responsible for the major complications of the disease. • Clinical disease associated with non-toxin-producing strains is generally milder. DR (MRS) M.B. FETUGA
CLINICAL FEATURES • The incubation period of diphtheria is 2–5 days (range, 1–10 days). • Disease can involve almost any mucous membrane. The features depend on the sites of infection. • For clinical purposes, it is convenient to classify diphtheria into a number of specific manifestations, depending on the site of disease. DR (MRS) M.B. FETUGA
ANTERIOR NASAL DIPTHERIA • The onset is indistinguishable from that of the common cold and is usually characterized by a mucopurulent nasal discharge (containing both mucus and pus). This discharge may become blood-tinged. • A white membrane usually forms on the nasal septum. • The disease is usually fairly mild because of apparent poor systemic absorption of toxin in this location. It can thus be terminated rapidly by antitoxin and antibiotic therapy. DR (MRS) M.B. FETUGA
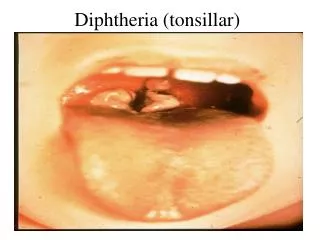
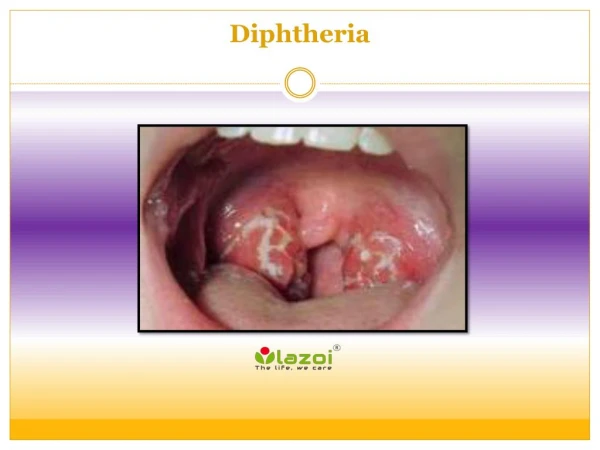
PHARYNGEAL OR TONSILAR DIPTHERIA • The most common sites of infection (>90%) are the pharynx and the tonsils. • Infection at these sites is usually associated with substantial systemic absorption of toxin. • The onset of pharyngitis is insidious. Early symptoms include malaise, sore throat, anorexia, and low-grade fever. DR (MRS) M.B. FETUGA
PHARYNGEAL OR TONSILAR DIPTHERIA Within 2–3 days, a bluish-white membrane forms over the tonsil and soft palates. Over time, the colour of the membrane changes to greyish-green. There is a minimal amount of mucosal erythema surrounding the membrane. The membrane is adherent to the tissue, and forcible attempts to remove it cause bleeding. Extensive membrane formation may result in respiratory obstruction. DR (MRS) M.B. FETUGA
PHARYNGEAL OR TONSILAR DIPTHERIA • The patient may recover at this point; or if enough toxin is absorbed, develop severe prostration, pallor, tachycardia, stupor, coma, and may die within 6 to 10 days. • Patients with severe disease may develop marked edema of the submandibular areas and the anterior neck along with lymphadenopathy, giving a characteristic “bull neck” appearance. DR (MRS) M.B. FETUGA
LARYNGEAL DIPTHERIA • Laryngeal diphtheria can be either an extension of the pharyngeal form or the only site involved. • Symptoms include fever, hoarseness, and a barking cough. The membrane can lead to airway obstruction, coma, and death. DR (MRS) M.B. FETUGA
CUTANEOUS DIPTHERIA • Usually a mild form of the disease. • Skin infections are quite common in the tropics and are probably responsible for the high levels of natural immunity found in these populations. • Skin infections may be manifested by a scaling rash or by ulcers with clearly demarcated edges and membrane. DR (MRS) M.B. FETUGA
COMPLICATIONS • Myocarditis • Neuritis most often affects motor nerves and usually resolves completely. • Paralysis of the soft palate (nasal regurgitation and nasal voice) is most frequent during the third week of illness. • Blurred vision from oculomotor paralysis • Limb paralysis indistinguishable from Guillain Barre Syndrome. • Diaphragmatic paralysis and respiratory failure. • Thrombocytopaenia & proteinuria(renal) DR (MRS) M.B. FETUGA
PROGNOSIS The overall case-fatality rate for diphtheria is 5%–10%. Higher death rates (up to 20%) occur among the under-fives. DR (MRS) M.B. FETUGA
LABORATORY DIAGNOSIS • Culture of the lesion is done to confirm the diagnosis. It is critical to swab the pharyngeal area, especially any discolored areas, ulcerations, and tonsillar crypts. • Culture medium containing tellurite is preferred to Loeffler’s because it provides a selective advantage for the growth of this organism. A blood agar plate is also inoculated for the detection of hemolytic streptococcus. If diphtheria bacilli are isolated, they must be tested for toxin production. DR (MRS) M.B. FETUGA
LABORATORY DIAGNOSIS • Polymerase Chain Reaction may also be used in the presence of non-viable diphtheroids. • In the event that prior antibiotic therapy may have impeded a positive culture in a suspect diphtheria case, two sources of evidence may aid presumptive diagnosis: (1) isolation of C. diphtheriae from close contacts, and/or (2) a low non-protective diphtheria antibody titer in sera obtained prior to antitoxin administration (less than 0.1 I.U.). DR (MRS) M.B. FETUGA
DIFFERENTIAL DIAGNOSIS • Bilateral parotitis • Streptococcal pharyngitis • Epiglottitis • Acute Laryngotracheobronchitis • Vincent angina- (necrotizing gingivitis- anaerobe • Non-specific cervical adenitis • Cystic hygroma • Branchial cysts DR (MRS) M.B. FETUGA
MANAGEMENT Diphtheria Anti-toxin • Diphtheria antitoxin, produced in horses, provides passive immunity since it contains antibodies against the antigens of the toxins. • Antitoxin will not neutralize toxin that is already fixed to tissues, but will neutralize circulating (unbound) toxin and will prevent progression of disease. Therefore, the anti-toxin should be promptly administered once diphtheria is suspected DR (MRS) M.B. FETUGA
MANAGEMENT Diphtheria anti-toxin: • It is preferably given intravenously (after a test dose) at a dose which depends on the site and severity (10,000 – 20,000 units for nasal; 20,000 – 40,000 units for pharyngeal; 60,000 – 80,000 units for extensive disease. • Respiratory support and airway maintenance should also be administered as needed. DR (MRS) M.B. FETUGA
MANAGEMENT • Antibiotics • Erythromycin orally or by injection (40 mg/kg/day in 4 divided doses) for 14 days, • Procaine penicillin G daily, intramuscularly (100,000 U/ kg/ day in 4 divided doses) for 14 days. • The disease is usually not contagious 48 hours after antibiotics are instituted. • Elimination of the organism should be documented by two consecutive negative cultures after therapy is completed. DR (MRS) M.B. FETUGA
OTHER SUPPORTIVE MANAGEMENT • Mandatory bed rest • Respiratory supports • Oxygen therapy • Endotracheal intubation • Tracheostomy • Nasogastric feeding in cases of palatal paralysis. DR (MRS) M.B. FETUGA
PREVENTIVEMEASURES • Protection with the triple vaccine DPT (or DTaP) which contains the diphtheria toxoid is recommended for administration in 3 doses at 6, 10 and 14 weeks of life. • The toxoid has an estimated clinical efficacy of about 97%. DR (MRS) M.B. FETUGA
PREVENTIVE MEASURES • For close contacts, especially household contacts, a diphtheria booster, appropriate for age, should be given. • Contacts should also receive antibiotics—benzathine penicillin G (100, 000u/ kg/ day) or a 7- to 10-day course of oral erythromycin, (40 mg/kg/day for children and 1 g/day for adults). DR (MRS) M.B. FETUGA