Download
1 / 49
500 likes | 641 Views
Exercise Prescription for Aerobic Training in the Cardiac Population. Teresa Eber Lee, EdD, RCEP, CCRP, Wellcoach Program Director Clinical Exercise Science Winona State University. Are there people who should not exercise?. Unstable angina

E N D
Exercise Prescription for Aerobic Training in the Cardiac Population Teresa Eber Lee, EdD, RCEP, CCRP, Wellcoach Program Director Clinical Exercise Science Winona State University
Are there people who should not exercise? • Unstable angina • Uncontrolled HTN (180/110 mm Hg), dysrhythmias, or DM • Uncompensated heart failure • Severe aortic stenosis • Active pericarditis or myocarditis • Acute thrombophlebitis or recent PE • 2nd or 3rd degree heart block without a pacemaker • Electrolyte abnormalities (hypo/hyperkalemia)
What are your goals when prescribing exercise? Prescribe a program that: • Promotes positive physiological changes • Is safe and avoids injuries • Fosters exercise adherence
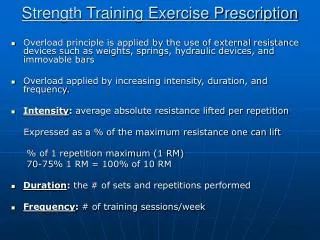
Principals of Exercise Prescription FITT-VP Principle
Frequency • Minimally 3 day/week • Preferably >5 days/week • 3 supervised sessions • 2 or more sessions on their own • “most days of the week”
Time / Duration • 20 - 60 minutes of continuous activity • shoot for 30 – 40 minutes • reduces boredom • less chance for injury
“walk often and walk far” Ades et al., Circulation: 2009 • Standard Cardiac Rehabilitation • 3 days week • 25-40 minutes/session • 65-75% peak VO2 • goal of 1200-1500 kcal/week • High Caloric Exercise for Cardiac Patients • 5-7 days week • 45-60 minutes/session • 50-60% peak VO2 • goal of 3,000-3,500 kcal/week
High Caloric Standard CR Kcal/day 615 269 Kcal/wk 3037 807 Weight Loss (kg) 8.2 3.7 Waist Loss (cm) 7 5 MET Syndrome (%) 47 17 Results – 5 months
Type or Modality • Any large muscle, sustainable activity is acceptable (rhythmic) • Modes with an upper body component may have some advantages: • increased upper body muscular endurance • sharing of workload, so can do more work at same perceived effort (RPE); burn more calories • may facilitate glucose metabolism
Changes in aerobic capacity following 12 weeks of stationary cycling, treadmill walking, stepping, or simulated cross-country skiing VO2max (ml/kg/min) Control Bike Tmill Stepper Skier
Changes in body weight and % fat following 12 weeks of stationary cycling, treadmill walking, stepping, or simulated cross-country skiing. Stepper Skier Control Bike Tmill Change
SPECIFICITY SAID PRINCIPLE Specific Adaptation to Imposed Demands
Intensity • If you have an maximal effort graded exercise test (GXT): • 40 - 80% of VO2peak or Heart Rate Reserve (Karvonen)
HR/VO2 Relationship 40-80% Divide VO2 (ml/kg/min) by 3.5 = METs
Exercise Prescription by METs40-80% of VO2max or max METs • 1 MET = 3.5 ml/kg/min = amount of oxygen the average person consumes at rest. • Someone with a maximal capacity of 10 METs has a capacity that is 10 times greater than their resting level. • If I want someone to work at 40-60% of maximal METs: • 10 METs X .40 = 4 METs • 10 METs X .60 = 6 METs
40-80% of Heart Rate Reserve (aka: Karvonen Method) • Target HR = [(max HR - rest HR) X desired % + rest HR] Lower Limit Upper Limit Maximal heart rate 180 180 Resting heart rate - 60 - 60 Heart rate reserve 120 120 Desired % X .40 X .60 48 72 Resting heart rate + 60 + 60 108 132
Signs and Symptoms Below Which an Upper Limit for Exercise Intensity Should be Set Angina Drop in SBP Significant ST depression on previous GXT Increased frequency of ventricular ectopy Onset of heart blocks (e.g., BBBs, 2º or 3º AV block) Other signs/symptoms of intolerance to exercise (e.g., extreme SOB) **Exercise heart rate should be set at least 10 bpm below the HR associated with any of the above criteria
RPE Method (Borg Scales) 6 - 20 Scale1 - 10 Scale 6 0 7 Very, very light 0.5 Extremely weak 8 1 Very weak 9 Very light 2 Weak 10 3 Moderate 11 Fairly light 4 12 5 Strong 13 Somewhat hard 6 14 7 Very strong 15 Hard 8 16 9 17 Very hard 10 Very, very strong 18 19 Very, very hard 20
What about the Cardiac Meds? 19 No BB 17 13 10 8 BB RPE 13 No BB: 135/155 = 87% On BB: 115/130 = 87%
Exercise Prescription with or without a GXT • Frequency: same • Time / duration: same • Modalities: same • The only difference is how you prescribe exercise intensity!
Intensity If you do not have an exercise test: AACVPR 2 - 4 METs 11 - 14 RPE ACSM Rest +20bpm to + 30 bpm (arbitrary upper limit) RPE 12-16 To tolerance if asymptomatic <10 beat below ischemic and angina threshold
If you use RPE only…you still record the exercise HRs on each modality to get an idea of what they are • That allows you to recognize deviations from that, which may indicate: • some sort of dysrhythmia • heart block • forgot to take their meds
Yes…Yes…Yes • ACSM • 20-30 bpm are “arbitrary upper limits” • RPE 13-16 on a 6-20 scale • “to tolerance if asymptomatic” • AACVPR • “Over time, stable patients typically progress to exercise plans similar to those presented in Table 8.6.” • RPE of 11-16 (which corresponds to 40-80% of HR reserve)
Titrate workloads based on: • Signs and symptoms • EKG and BP responses • RPE • Talk Test • Staff comfort • Sound clinical judgment
Talk Test Exercise at an intensity where you can still carry on a “normal” conversation!
In subjects who had exertional ischemia, 18/19 subjects were below the ischemic threshold when they could still pass the Talk Test. Ischemia did not occur until after they could no longer speak comfortably.
Tim McConnell DataGeisinger Medical Center Week 1Week 12 Exercise HR GXT 99 99 No GXT 97 103 Exercise METs GXT 3.2 3.8 No GXT 2.8 3.7 **No difference in complication rates during training between groups and all problems were minor (e.g., dysrhythmias, hypotension)
Progression • Depends upon: • 1. Functional capacity - lower go slower • 2. Age - older takes longer • 3. Health status – co-morbidities may • affect how fast you can progress • 4. Goal - what do they want to do? • As a general rule, increase duration first and then alter intensity.
End of Cardiac Rehab • Cardiovascular Stress Test (CVST) • Non-diagnostic, functional capacity test • Guidelines for home exercise program.
EXERCISE PRESCRIPTION for 1. MODE: Aerobic Exercise: walk, bike, etc. Strength Training: weights or therabands Stretching • FREQUENCY: Aerobic Exercise: 5-7 days a week Stretching: after each workout Strength training: 2-3 days a week - 3. DURATION: 30-60minutes of continuous aerobic exercise Warm-up for 5 minutes at a slow pace Cool-down for 5 minutes at a slower pace 4. INTENSITY: Rate of Perceived Exertion: (RPE) 11-15 “Fairly Light to Hard” Heart Rate Range: 72-66 beats per minute 11-12 Beats in a 10 second count Remember to adjust your workload to meet your prescribed exertion. Stop exercise if at any time you feel chest pain, excessive shortness of breath, dizziness, light-headedness, excessive sweating, frequently skipped beats or blurred vision. ______________ , congratulations on making healthy lifestyle change! Remember, consistent exercise is the key to maintaining good health. Continue to exercise, eat healthy, and be good to yourself. If you have any questions or need anything, please call us or stop by the Exercise Center. 775-2955
Home Program • No insurance coverage • Co-pay • Back to work • Driving issues
Home Program • Review cardiovascular exercise that can be done at home with minimal equipment. • 5-7 days per week • RPE 11-13 or target heart rate if applicable • 30-60 minutes daily • Progression • Stretches following exercise. • Exercise log given to track progress.
Follow-up • Every 1-2 weeks • Introduce strength training • 2-3 days per week using therabands. • 1-2 sets, 8-12 reps
Case Studies • Patient History: • 55 year old male. • S/P MI and Stent to LAD • BMI 34 • GXT Bruce Protocol: • 8 METS • HRrest 62 bpm • HRmax 136 bpm • No Ischemia or Angina • What goal would you recommend for rehabilitation? • What is his HR reserved? • What mode of exercise do you recommend? • What is an appropriate THR?
Case Studies • Patient Hx: • 62 y/old Female • Stable Angina • GXT Naughton Protocol • 4.8 Mets • HRrest 74 bpm • HRmax 115 bpm • Angina and 1mm ST • HR of 108 bpm • BP of 146/74 • Is this patient Safe to exercise in a CR program? • What was the Rate Pressure Produce at the time of ischemia? • What intensity would you use for the ExRx?
Case Studies • Patient History: • 67 year old male. • S/P CABG (1 month ago) • No GXT: • HRrest 58bpm • BP 118/66 • No angina • No physical limitations? • What intensity would you start this patient? • How would you progress?