Download
1 / 47
860 likes | 3.07k Views
PLACENTA PREVIA. PRESENTED BY: JISHA MARIA LR/DR DEPARTMENT. DEMOGRAPHIC DATA. NAME : MS. P.A. AGE: 47/F. CASE NO: 193***. Dx: G9P7A1 29 weeks + 3 days, PTL T/C Placenta Previa, Previous LCCS. PHYSICAL ASSESSMENT. GENERAL. The patient is 47 y/o, FEMALE, weight 74 kg.

E N D
PLACENTA PREVIA PRESENTED BY: JISHA MARIA LR/DR DEPARTMENT
NAME: MS. P.A. AGE: 47/F CASE NO: 193*** Dx: G9P7A1 29 weeks + 3 days, PTL T/C Placenta Previa, Previous LCCS
GENERAL • The patient is 47 y/o, FEMALE, weight 74 kg. • She is conscious, coherent • With the following Vital Signs: • BP= 120/80 mmHg • PR=72 bpm • RR= 23 /cpm • Temp=36.8⁰C
SKIN • Pallor of skin and nails • No palpable masses or lesions
HEAD • Maxillary, frontal, and ethmoid sinuses are not tender • No palpable masses or lesions • No areas of deformity
LOC & ORIENTATION • Awake and alert • Oriented to Persons, Place, Time
EYES • Pale conjunctivae and no dryness • Pupils equally round and reactive to light
EARS • No unusual discharges noted
NOSE • Pink nasal mucosa • No unusual nasal discharge • No tenderness in sinuses
MOUTH • Dry mouth and lips • Free of swelling and lesions
NECK AND THROAT • No palpable lymph nodes • No masses and lesions seen
CHEST AND LUNGS • Symmetrical chest wall upon movement • Clear breath sounds • Absence of chest pain
HEART • Regular rhythm
ABDOMEN • Abdomen is soft • With mild to moderate uterine contraction • With mild hypogastric pain
ABDOMEN • With active bowel sounds • No abdominal tenderness
GENITOURINARY • No discharges or foul smell • With minimal vaginal spotting up to 2-13 pads per day • Able to void freely • No pain in urination
EXTREMITIES • Pulse full and equal • No lesions noted
PAST MEDICAL HISTORY • With history of Abortion At 3 yr before • With 5 times Surgical history of LSCS
PRESENT MEDICAL HISTORY C/O: Mild Hypogastric Pain MEDICAL HISTORY:G9P7A1 29 3/7 weeks Age of Gestation ON EXAMINATION: BP: 120/80mmHg, PR: 72 bpm, RR: 23 cpm, Temp. 36.8 ⁰C • LMP: Unknown • PV not done • No allergies to any food or drug • With Hypertensive and Diabetic parents
INVESTIGATIONS: • Ultrasonographic Result • PU 31weeks + 5days AOG by fetal biometry • Live Singleton in cephalic presentation, Male fetus • Good Cardiac and somatic activity • Left Lateral Placenta, Grade II, Previa Totalis • Adequate fluid volume BPP= 8/8
INVESTIGATIONS: • MRI Result: Pelvis shows gravid uterus with singlefetus and the placenta is in left lateral position and in lower uterine segment completely covering the internal os and shows heterogenoussigal intensity with bulging of lower uterine segment and irregular thick intraplacental T2 dark bands and loss of thin subplacentalmyometrial zone and tenting of the urinary bladder seen along its ntero-superior margin, most probably suggestive of placenta previa.
INTRODUCTION • The term placenta previa refers to a placenta that overlies or is proximate to the internal os of the cervix. The placenta normally implants in the upper uterine segment. In placenta previa, the placenta either totally or partially lies within the lower uterine segment. Traditionally, placenta previa has been categorized into 4 types: • Complete placenta previa • where the placenta completely covers the internal os. • Partial placenta previa • where the placenta partially covers the internal os. Thus, this scenario happens only when the internal os is dilated to some degree. • Marginal placenta previa • which just reaches the internal os, but does not cover it. • Low lying placenta • which extends into the lower uterine segment but does not reach the internal os.
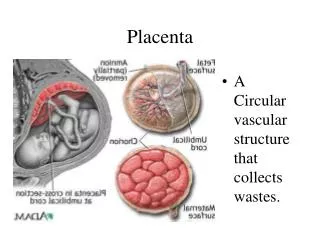
The placenta signifies the "second" or "embryonic" period of pregnancy (after the implantation period) and describes the establishment of a fully functional placenta. The placenta is an apposition of foetal and parental tissue for the purposes of physiological exchange. There is little mixing of maternal and foetal blood, and for most purposes the two can be considered as separate. • The placenta can be thought of as a "symbiotic parasite", unique to mammalia. The placenta provides an interface for the exchange of gases, food and waste. It also facilitates the de novo production of fuel substrates and hormones and filters potentially toxic substances. • The placenta has two distinct seperate compartments; the fetal side consisting of the trophoblast and chorionic villi and the maternal side consisting of the decidua basalis.
The placenta consists of a foetal portion formed by the chorion and a maternal portion formed by the decidua basalis. The uteroplacental circulatory system begins to develop from approximately day 9 via the formation of vascular spaces called "trophoblastic lacunae". • Maternal sinusoids develop from capillaries of the maternal side which anastamose with these trophoblastic lacunae. The differential pressure between the arterial and venous channels that communicate with the lacunae establishes directional flow from the arteries into the veins resulting in a uteroplacental circulation.
Placental Blood Supply • Maternal blood carrying oxygen and nutrient substrate to the placenta must be transferred to the fetal compartment and this rate of transfer is the rate limiting step in the process. Therefore the placenta has a significant blood to facilitate improved exchange. • Fetal blood enters the placenta via a pair of umbilical arteries which have numerous branches resulting in fetal chorionic villi within the placenta, terminating at the chorionic plate. The fetal chorionic villi are then surrounded by maternal tissues. This physiology is referred to as "invasive decidualisation" as the fetal chorionic villi effectively invade the maternal tissues. Invasive decidualisation is not present in pigs or sheep.
Placental Blood Supply • Oxygen and nutrient rich blood returns to the fetus via the umbilical vein. Maternal blood is supplied to the placenta via 80-100 spiral endometrial arteries which allow the blood to flow into intervillous spaces facilitating exchnage. The blood pressure within the spiral arteries is much higher than that found in the intervillous spaces resulting in more efficient nutrient exchange within the placenta.
ETIOLOGY • Increased maternal age • Uterine factors: • Previous CS • Instrumentation of the uterine cavity (D and C for miscarriages or Induced Abortions) • Placental factors: • Multiparity • Cigarette smoking • Living at high altitude
SIGNS AND SYMPTOMS • Vaginal bleeding • Painless but can be associated with uterine contractions and abdominal pain • Bleeding may range from light to severe • Gross hematuria
INTERVENTION • Bed rest in lateral position to maximize venous return and placental perfusion • Women in the third trimester are advised to avoid sexual intercourse and exercise and to reduce their activity level
TREATMENT Depends upon the extent and severity of bleeding, the gestational age and condition of the fetus, position of the placenta and fetus and whether the bleeding has stopped. • Caesarean section – as soon as he baby can be safely delivered (typically after 36weeks gestation). Although emergency CS at any earlier gestational age may be necessary for heavy bleeding that cannot be stopped. • Hysterectomy
COMPLICATIONS Maternal: • Increased risk of PROM leading to premature labor • Immediate hemorrhage with possible shock and maternal death • Postpartum hemorrhage • Placenta Accreta • Accreta Vera – a term used to denote a placenta with villi that adhere to the superficial myometrium • Increta – when the villi adheres to the body of the myometrium, but not through its full thickness • Percreta – when the villi penetrate the full thickness of the myometrium and may invade neighboring organs such as the bladder or the rectum
Fetal: Abnormal fetal presentation (breech) Reduced fetal growth Prematurity
PRIORITIZATION OF NURSING PROBLEMS • Impaired fetal gas exchange related to altered blood flow and decreased surface area of gas exchange at site of placental detachment • Ineffective Tissue Perfusion related to excessive bleeding causing fetal compromise • Deficient Fluid Volume related to excessive bleeding • Anxiety related to excessive bleeding, procedures, and possible fetal-maternal complications
CONCLUSION • Presented a case of a 47 y/o Multigravida, G9P7A1, with pregnancy 29 wks + 3 days with PTL t/c PLACENTA PREVIA, Previous LSCS • The treatment depends upon the extent and severity of bleeding, the gestational age and condition of the fetus, position of the placenta and fetus and whether the bleeding has stopped. • Placenta Previa is a medical emergency that needs immediate management because it can lead to serious maternal and fetal complications, even death of one or both of them. • Nurse-led patient education and the provision of a supportive environment are essential to the optimal management of Placenta Previa • Individually tailored and compassionate nursing care of women with Placenta Previa will serve to enhance the wellbeing of mother and baby