Download
1 / 1
40 likes | 476 Views
Implications of the SOGC Clinical Practice Guideline, “Vaginal Delivery of Breech Presentation” Dr. Cara Janzen, MD, Mr. Tyler Williamson, BSc. Dr. Sue Ross, PhD Department of Family Medicine, The University of Calgary. Introduction. Methods. Results.

E N D
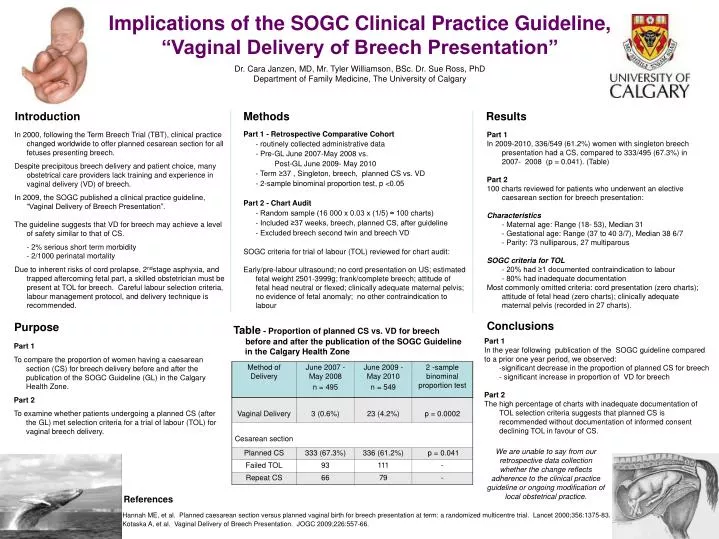
Implications of the SOGC Clinical Practice Guideline, “Vaginal Delivery of Breech Presentation” Dr. Cara Janzen, MD, Mr. Tyler Williamson, BSc. Dr. Sue Ross, PhD Department of Family Medicine, The University of Calgary Introduction Methods Results In 2000, following the Term Breech Trial (TBT), clinical practice changed worldwide to offer planned cesarean section for all fetuses presenting breech. Despite precipitous breech delivery and patient choice, many obstetrical care providers lack training and experience in vaginal delivery (VD) of breech. In 2009, the SOGC published a clinical practice guideline, “Vaginal Delivery of Breech Presentation”. The guideline suggests that VD for breech may achieve a level of safety similar to that of CS. - 2% serious short term morbidity - 2/1000 perinatal mortality Due to inherent risks of cord prolapse, 2ndstage asphyxia, and trapped aftercoming fetal part, a skilled obstetrician must be present at TOL for breech. Careful labour selection criteria, labour management protocol, and delivery technique is recommended. Part 1 In 2009-2010, 336/549 (61.2%) women with singleton breech presentation had a CS, compared to 333/495 (67.3%) in 2007- 2008 (p = 0.041). (Table) Part 2 100 charts reviewed for patients who underwent an elective caesarean section for breech presentation: Characteristics - Maternal age: Range (18- 53), Median 31 - Gestational age: Range (37 to 40 3/7), Median 38 6/7 - Parity: 73 nulliparous, 27 multiparous SOGC criteria for TOL - 20% had ≥1 documented contraindication to labour - 80% had inadequate documentation Most commonly omitted criteria: cord presentation (zero charts); attitude of fetal head (zero charts); clinically adequate maternal pelvis (recorded in 27 charts). • Part 1 - Retrospective Comparative Cohort • - routinely collected administrative data • - Pre-GL June 2007-May 2008 vs. • Post-GL June 2009- May 2010 • - Term ≥37 , Singleton, breech, planned CS vs. VD • - 2-sample binominal proportion test, p <0.05 • Part 2 - Chart Audit • - Random sample (16 000 x 0.03 x (1/5) ≈ 100 charts) • - Included ≥37 weeks, breech, planned CS, after guideline • - Excluded breech second twin and breech VD • SOGC criteria for trial of labour (TOL) reviewed for chart audit: • Early/pre-labour ultrasound; no cord presentation on US; estimated fetal weight 2501-3999g; frank/complete breech; attitude of fetal head neutral or flexed; clinically adequate maternal pelvis; no evidence of fetal anomaly; no other contraindication to labour Conclusions Purpose Table - Proportion of planned CS vs. VD for breech before and after the publication of the SOGC Guideline in the Calgary Health Zone Part 1 In the year following publication of the SOGC guideline compared to a prior one year period, we observed: -significant decrease in the proportion of planned CS for breech - significant increase in proportion of VD for breech Part 2 The high percentage of charts with inadequate documentation of TOL selection criteria suggests that planned CS is recommended without documentation of informed consent declining TOL in favour of CS. Part 1 To compare the proportion of women having a caesarean section (CS) for breech delivery before and after the publication of the SOGC Guideline (GL) in the Calgary Health Zone. Part 2 To examine whether patients undergoing a planned CS (after the GL) met selection criteria for a trial of labour (TOL) for vaginal breech delivery. We are unable to say from our retrospective data collection whether the change reflects adherence to the clinical practice guideline or ongoing modification of local obstetrical practice. References Hannah ME, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomized multicentre trial. Lancet 2000;356:1375-83. Kotaska A, et al. Vaginal Delivery of Breech Presentation. JOGC 2009;226:557-66.