Download
1 / 39
1.14k likes | 5k Views
Common Nutritional problems in Bangladesh Part I. Dr. Mohammad Hayatun Nabi MPH(Aus), MHSM(Aus), MBBS Dept. of Public Health. Introduction. The prevalence of malnutrition in Bangladesh is among the highest in the world.

E N D
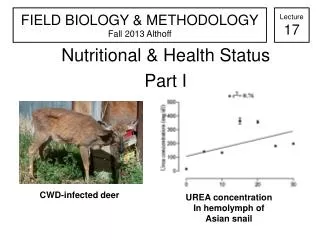
Common Nutritional problems in Bangladesh Part I Dr. Mohammad HayatunNabi MPH(Aus), MHSM(Aus), MBBS Dept. of Public Health
Introduction • The prevalence of malnutrition in Bangladesh is among the highest in the world. • Millions of children and women suffer from one or more forms of malnutrition including low birth weight, wasting, stunting, underweight, Vitamin A deficiencies, iodine deficiency disorders and anemia. • Globally, malnutrition is attributed to almost one-half of all child deaths. Dr. Mohammad Hayatun Nabi
Bangladesh has made good progress in the past decade to achieve Millennium Development Goal 1, the eradication of extreme poverty and hunger, more needs to be done. • Malnutrition rates have seen a marked decline in Bangladesh throughout the 1990s, but remained high at the turn of the decade. • Nationally, 41% of children under five years are moderately to severely underweight and 43.2% suffer from moderate to severe stunting, an indicator for chronic malnutrition. Dr. Mohammad Hayatun Nabi
Common Nutritional Problems • Protein energy malnutrition • Low birth weight • Nutritional anemia • Nutritional blindness • Iodine deficiency disorders • Seasonal vitamin deficiency Dr. Mohammad Hayatun Nabi
PEM- Introduction • Protein Energy Malnutrition (PEM) continues to be a major public health problem in many developing countries. • It affects mostly children under 5 years of age belonging to the poor underprivileged communities. • The condition is particularly serious during the post weaning stage and is often associated with infection. Dr. Mohammad Hayatun Nabi
Cont… • Respiratory infection and diarrhea are the common diseases that precipitate severe PEM and death. • Apart from contributing to high mortality, severe malnutrition can lead to permanent squeal in those who survive. • These include stunted growth, poor learning ability and reduced work efficiency. Dr. Mohammad Hayatun Nabi
“PEM”: Invariably reflects combined deficiencies in… • Protein: deficit in amino acids needed for cell structure, function • Energy: calories (or joules) derived from macronutrients: protein, carbohydrate and fat • Micronutrients: vitamin A, B-complex, iron, zinc, calcium, others Dr. Mohammad Hayatun Nabi
Classification • Several methods have been suggested for the classification of PEM. • The choice of classification depends on the purpose for which it is used. • In clinical studies, patients with severe PEM are classified into 3 groups- kwashiorkor, marasmus and marasmic kwashiorkor. • WHO classification • Gomez classification • Wellcome classification Dr. Mohammad Hayatun Nabi
Gomez Classification Malnutrition Body weight (% of standard*) Grade 1 76-90 Grade 2 60-75 Grade 3 <60 *Harvard standard Dr. Mohammad Hayatun Nabi
Etiology • Protein energy malnutrition results from the interaction of several factors of which, inadequate diets and infectious diseases are the most important. • Preschool children age are most seriously affected because their nutritional requirements are relatively higher than those of adults and infections occur more frequently in this age group. Dr. Mohammad Hayatun Nabi
Etiology • Diet • Free radicals • Infections • Socio-demographic factors Dr. Mohammad Hayatun Nabi
Marasmus • Clinical features: • •Severely wasted (emaciated) & stunted •“Balanced”starvation • •“Old Man”face, wrinkled appearance, sparse hair • •No edema, fatty liver, skin changes • •Too little breast milk or complementary foods • <2yrs of age Dr. Mohammad Hayatun Nabi
Dilute and unhygienic formula or bottle feeding Too little breast milk, often after 6 mo of age Dr. Mohammad Hayatun Nabi
•Kwashiorkor • Clinical Features: • Edema, it tends to be generalised • •Mental changes • •Hair changes: the black color alters to blonde, grey • Mucosal changes: angular stomatitis • •Fatty liver • •Dermatosis (skin lesions) • •Infection • Anorexia • •High case fatality • •Low prevalence • 1st to 3rd yrs of life Dr. Mohammad Hayatun Nabi
Differences between Marasmus and Kwashiorkor Dr. Mohammad Hayatun Nabi
Differences between Marasmus and Kwashiorkor Dr. Mohammad Hayatun Nabi
Prevention of PEM • Prevention of Kwashiorkor • Educate mother • Advice to farmers • Provide food supplements in hospitals • Legumes, nuts and seeds (locally produced) • Prevention of Marasmus • Family planning • Immunization program • Encourage breastfeeding • Maternity and child health clinics Dr. Mohammad Hayatun Nabi
Vitamin A deficiency Disorders Dr. Mohammad Hayatun Nabi
Introduction • Nutritional blindness due to xeropthalmia is an important public health problem among young children in developing countries. • The term xerophthalmia encompasses all ocular manifestations of vitamin A deficiency. It includes the structural changes affecting conjunctiva, cornea and occasionally retina, and also the biophysical disorders of retinal rod and cone functions. Dr. Mohammad Hayatun Nabi
Vitamin A Adequacy Deficiency Bone growth Growth retardation Reproduction Dysfunction (M&F) Embryogenesis Teratogenesis Rod vision Night blindness Cell differentiation Epithelial metaplasia Immunity Impaired innate & acquired defenses Dr. Mohammad Hayatun Nabi
VITAMIN A DEFICIENCY DISORDERSHealth Consequences of VAD • Xerophthalmia: Mild to severe • Corneal blindness and disability • Anemia • Stunted growth • Impaired immunity • Increased severity of infection (eg,measles, diarrhea, or malaria) • Mortality Dr. Mohammad Hayatun Nabi
WHO Xerophthalmia Classification (1982) • XN Nightblindness • X1A Conjunctival xerosis • X1B Bitot’s spots • X2 Corneal xerosis • X3 Corneal ulceration • Keratomalacia • XS Corneal scarring • XF Xerophthalmic fundus Dr. Mohammad Hayatun Nabi
Night Blindness • It is an useful screening tool and correlates with other evidence of vitamin A deficiency. • It can be elicited in the case of young children by detailed questioning of the parents or the guardians. • The children usually cannot see in dim light, either at dusk or down. • The value of night blindness will depend on the care with which the questions are asked, and upon the degree to which the phenomenon of night blindness is recognized by the community. Dr. Mohammad Hayatun Nabi
Magnitude • Globally it is estimated that every year about 7,00,000 children are likely to develop corneal lesions due to vitamin A deficiency. • The problem is considered to be of public health significance in 36 countries, in South East Asia, the western Pacific and Africa. • About 20-40% million children are estimated to have mild vitamin A deficiency at any point of time. Mahtab et al, 2003 Dr. Mohammad Hayatun Nabi
Epidemiology Age Vitamin A deficiency is preponderant in children. While it is rare during infancy, preschool age children are at a greater risk. SexXerophthalmia is more frequent in boys than in girls.The incidence of keratomelacia is similar in both the sexes. Socio-economic FactorsChildren from rural and tribal families belonging to low-income group are more vulnerable to vitamin A deficiency.The mothers of vitamin deficient children are generally illiterate and unaware of the importance of diet in disease.Because of food fads and false beliefs, foods like colostrums, green leafy vegetables and papaya which are rich in vitamin A are avoided. Dr. Mohammad Hayatun Nabi
Seasonal Effects • The seasonal changes in vitamin A deficiency are related to times of harvest. • The highest prevalence is observed in the months of May-June and November-December. Drought • The extent of vitamin A deficiency is more during drought due to non-availability of leafy vegetables because of shortage of rainfall. • The prevalence is higher in areas which are chronically drought prone. Dr. Mohammad Hayatun Nabi
Aetiology • Inadequate dietary intake of vitamin A or its precursor (b-carotine) is the most important contributory factor. • The common childhood infections like measles, diarrhea, respiratory tract infections, and infestations like ascariasis and giardiasis interfere with the absorption of vitamin A. • Low purchasing power of the communities and their inability to meet the dietary requirements even after spending 80-90% of their income on food is an important factor for the widespread prevalence of vitamin A deficiency Dr. Mohammad Hayatun Nabi
Prevention And Control • Vitamin A deficiency is one of the simplest preventable nutritional disorders. • Several strategies are possible for controlling xerophthalmia and the consequent blindness: • Periodic dosing Supplies • Fortification • Dietary modifications to promote production and consumption of vitamin A/ beta carotene rich foods through nutrition education and/or horticulture intervention. Dr. Mohammad Hayatun Nabi
Thank You Dr. Mohammad Hayatun Nabi